The Fountain of Health: a First Principles Guide to Rejuvenation
I’d like to live in a world where age really is just a number. For the last ~3 years or so, I’ve been nerding out with increasing fervour about longevity biotech, having originally been inspired by one of Aubrey de Grey’s many interviews. I want to explain how and why I’ve become optimistic about the short-term prospects of indefinite healthy life extension, in terms of how I’ve come to think about ageing, disease, medicine and rejuvenation.
A revolution is underway in how people think about health and medicine. Worst case scenario, it will unlock a whole new generation of therapies that can actually cure chronic age-related diseases, instead of just moderately slowing their progression at the expense of multiple poorly understood side effects. Best case scenario, it will enable us to live indefinitely in bodies that are functionally and cosmetically indistinguishable to those of 25 year olds. As with AGI, nobody can predict with certainty how long this will take, but optimism has grown tremendously over the past five years, and it is no longer unusual to encounter experts who believe that the ageing process is malleable.
This timeframe depends massively on how rapidly we can divert funding and talent toward longevity biotechnology, because we are not going to achieve this outcome by doing more of what mainstream biomedicine has been doing. You could liken our position to where SpaceX are right now on the road to Mars: there’s a long way to go still, but no Nobel prizes are required, no major scientific breakthroughs, just a lot of engineering. In this post, I will explain what ageing is, why we suck so much at treating chronic illnesses, and how this problem will be solved by a new kind of medicine, one that directly modifies the structure of your body so as to make you healthier.
What is ageing?
In biology it is said that function follows form, and in fact this is true of all machines. Machines do the things they do because of the way they are set up, because of their shape, because of their structure.
Damage can be defined as any structural change that causes a loss of function.
Any machine will do damage to itself in the course of normal operation.
Ageing, then, is the process by which a machine loses function as a result of damage sustained from normal operation.
The human body is a machine. Biological ageing is a progressive loss of function caused by damage that the body does to itself.
Ageing is not a thing. There is no single process that is or causes ageing, it’s just the body gradually breaking itself in many different ways.
For this reason, I don’t actually use the word “ageing” very much internally—it seems confusing and unnecessary to me. If you damage a machine then by definition it won’t work as well as it did, and if you damage it too much then it’ll stop working altogether. Doesn’t matter if the damage is caused by something external or by the machine itself. The word “ageing” makes this sound more mysterious than it is, like there’s some separate magical phenomenon that causes organisms to slowly decay and die. Ageing is a mysterious answer to a mysterious question, and you could argue that it belongs in the same dustbin as phlogiston or elan vital.
I can grudgingly accept that we need a word for the general phenomenon by which people slowly decay and die with the passing of years, and ageing is that word. The problem is that it inclines us to imagine some single thing that causes decline. I’d accept “progressive loss of function due to intrinsic damage” as a reasonable definition of ageing, but only because it’s clear about cause and effect. If you go looking for ageing as a cause of functional decline then you will search forever, because you’re searching for something that doesn’t exist. There is no single branch of biology, no mechanism, no clock, no organ, no system, no molecule, no separable component of any kind that is primarily responsible for ageing. The war on ageing encompasses all aspects of biology, because ageing is the simultaneous damage and decline of all biological systems.
Needless to say, if your machine is malfunctioning, then to make it work properly again you must fix it. Sounds so obvious that it’s weird to even say it, right? And yet, when our bodies malfunction late in life, we mostly do not attempt to fix them. Instead, we try to treat the diseases themselves, almost like they were infectious diseases. We’ve been thinking by analogy, instead of from first principles. If we’re ever to make serious progress against the chronic diseases of old age, we have to stop treating disease, and start fixing damage.
Stem cell therapy is prototypical damage repair. Stem cell therapy is cool, exciting and controversial because it modifies the body’s structure directly—the damage repair paradigm simply extends this principle to all the other types of damage that fuck us up besides cell loss. Our oldest fields of medicine today (excepting surgery) are infectious disease and cancer. Cancer is very much like being infected by your own cells, so in both cases, we are fighting something other. But to defeat the pathologies of age, we must break the taboo against modifying old bodies to be more like young bodies, because the only difference between the bodies of old and young is that young bodies are healthier. Nobody really works on ageing, and nobody really works on longevity either—we work on health, of which longer life is but a side effect. There is no such thing as healthy ageing—psychological changes excepted, not one aspect of ageing is good for you. Biological ageing is loss of health.
What does it really mean to be healthy? What is health? My answer to that question is “the average 25 year old”. Being healthy means having a license to abuse your body and not pay for it the next day. Healthy bodies are better at homeostasis; they can tolerate greater perturbations from their set points and return to those set points faster. Healthy bodies have redundancy, they are robust, they are set up to tolerate certain amounts of damage without loss of function. They can move faster, think faster and heal faster. They can take more abuse, and don’t require careful management of sleep, diet and stress in order to function optimally. They rarely get sick. These are all things that we think of as “youth”, because they correlate so strongly with low chronological age that they might as well be the same thing. But they’re not.
Chronological age and ill health have progressed hand in hand for 100% of all humans who have ever lived. One consequence of this outrage is that age and sickness have become conflated in peoples’ minds, as have youth and health. The fountain of youth does not literally make people younger, because it is not a time machine. It makes people healthier. Normally when we think “health” we think “lifestyle”, but in the long run, lifestyle is something we do to preserve health, not restore it. Being healthy does not mean having a healthy lifestyle, it means having a body that is functional and robust. It’s about how big a hit you can take. Health is the absence of damage, ageing is the accumulation of damage, and rejuvenation is the reversal of damage, therefore healthcare without rejuvenation is grossly stunted. True healthcare is something we have never known.
Confusion about what ageing is, coupled with the extension of frailty that recent decades have brought us, has led to a common misconception known as the Tithonus fallacy. Apparently, people think you’re actually going to look and feel like you’re 150 when you’re 150. Hopefully the above paragraphs make it clear why this will not be the case: old people look and feel like shit because they are damaged and unhealthy, and this is the same thing that causes them to die. People don’t die because they get old, they die because they get sick. Perhaps the term “longevity” is problematic, by implying that we’re working specifically on making people live longer, as if we were going to cure all the diseases of ageing but leave ageing itself alone, condemning us to an indefinite future of frailty, tiredness and wrinklyness. But we’re not going to cure the diseases directly—that’s what we’ve been trying to do, and it hasn’t worked, as I will explain later. The only way to cure those diseases and significantly extend lifespan is to repair the underlying damage that causes them, and that damage is the only difference between an 80 year old body and a 25 year old body. I doubt it would be possible to keep people alive in a state of frailty much longer than we currently do, because it’s the frailty that kills them.

I don’t know how long it will take for rejuvenated people to start looking like 25 year olds. What I do know is that “25 year old bodies” is what we will start to approach asymptotically, once rejuvenation becomes the dominant field of biomedical research and medical practice. The better we get at fixing damage, the younger people will look when they step out of the rejuvenation clinic; it will be a world in which you get slowly healthier over time instead of sicker.
What is damage?
I defined damage as “any structural change that causes a loss of function”, and it’s important to recognize that this is a very broad definition. The words “damage” and “structure” tend to conjure the image of scratches, dents, cracks, erosion, “wear-and-tear”, disorder, loss of pattern. That’s what damage looks like in man-made machines, but in biological machines it’s quite different. A human is a machine made up of trillions of tiny robots called cells, each with a quasi-independent life of its own, which are constantly striving actively to maintain homeostasis. Arguably the biggest single difference between organisms and synthetic machines is that organisms are constantly repairing themselves.
This broad definition of damage can make it seem like I’m cheating somewhat. I’ve basically defined it in such a way that any change that makes people better when reverted automatically counts as damage. But this is precisely the strength of damage as a way of thinking: being defined counterfactually (damage is that which would improve function if it were repaired), it focuses the mind on what we can actually do that would make a difference. Identifying damage is the same thing as identifying therapeutic targets. To say that X caused Y is to say that Y would have gone differently if X were changed. Damage is thus defined as the root cause of pathology, as far upstream as it is possible to go without trespassing into the metabolic processes that cause damage. Judea Pearl would be proud.
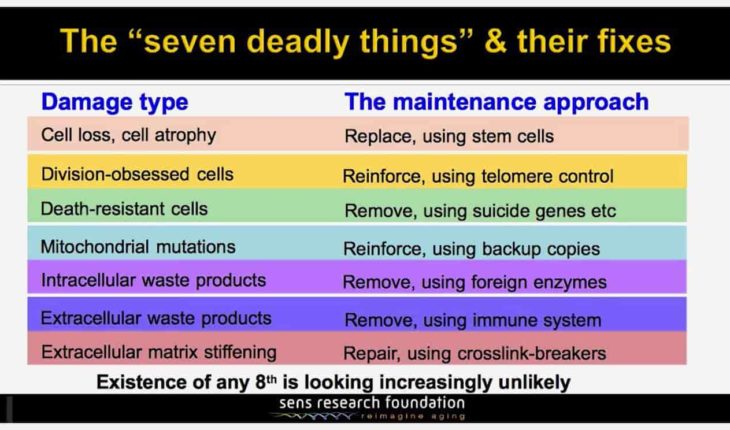
The taxonomy of damage shown above was proposed by Aubrey de Grey in 2001, and has become known as the SENS (Strategies for Engineered Negligible Senescence) approach to ageing. Importantly, it groups damage by the broad class of intervention required to fix it. Each damage type listed has many many sub-types within it, but they can all be fixed by similar means. If we can selectively destroy one type of slowly-accumulating bad cell then we can use similar means to destroy others; if we can discover enzymes that break down one type of intracellular junk and find a way to deliver those enzymes, then we can use the same approach on other types of junk.
Note also that 5 of the 7 damage types are all bad things that accumulate, such that “fixing” them simply means removing them. Reversing ageing can feel like an impossible task because we clearly lack the technology to manually put all the cells, molecules and atoms back in the right places as they become disarrayed, but the good news is that we don’t have to: they’re already really good at doing that themselves, so to a large extent we just need to remove the things that are stressing them out so they can do their jobs.
One of Aubrey’s more controversial claims is that this taxonomy is comprehensive, that is, all the damage we need to periodically fix to stay biologically young and stave death off indefinitely falls into one of these categories and is amenable to therapy. Diving into that claim in detail would require a whole separate essay (Aubrey wrote a whole book about it), but I’ll state my subjective assessment here. I have some niggling doubts about it, but I feel confident that it’s comprehensive enough that intervening in all seven categories will yield some level of unmistakable rejuvenation and healthy lifespan extension. If we make it that far, then it’s very unlikely that we’ll just stop and give up if it turns out there’s some other damage we need to fix, or if one of these categories turns out to be harder than we thought. As with all areas of technological development, the more we do it, the better we’ll get at it.
The other reason I don’t worry too much about the comprehensiveness of this taxonomy is that it’s kind of beside the point. The point is that damage repair is a revolutionary new approach to medicine, which is something we always want regardless of whether it’ll make us amortal or not. Few people believe it’s even possible for medicine to keep humans alive indefinitely, but that doesn’t stop us spending billions on Alzheimer’s research. Damage repair is just a better way of doing what we’re already trying to do.
You can’t stop it, but you can reverse it
Intuition dictates that you’ve got to walk before you fly. If ageing is advancing upon us like the out of control cruise ship in the movie Speed 2: Cruise Control, then surely we first have to slow it down before we stop it, and stop it before we can reverse it.
Intuitions can be misleading.
All seven damage types in the SENS platform are direct, unavoidable by-products of ordinary metabolism. Their accumulation can sometimes be slowed by living a healthier lifestyle, but they are present and ever-growing in all of us. Halting their accumulation altogether would require a radical redesign of how the human body works, and that is a much harder task than merely reversing said changes once they’ve already happened. The former requires us to redesign the human body into some novel architecture that somehow does not damage itself over time—and of course, this is no good for people who are already damaged and suffering today. But the latter only requires us to re-engineer the body back to a youthful structure, which we already know functions very efficiently.
Source: Aubrey de Grey
Note: T-headed arrows mean “inhibits”
This is the reason why I don’t cite research into calorie restriction, metformin, rapamycin, resveratrol, sirtuins or longevity genes as reasons to get excited. These interventions, which you might term the “gerontology” approach, all aim to modestly slow the ageing process, and the return on such investments, in terms of healthy years gained and suffering avoided, looks underwhelming to me. Not only that, but they sometimes feel a bit like voodoo, lacking a clear story as to how exactly such interventions should be expected to preserve function. Damage repair therapies aim to directly reverse changes that clearly cause problems, whereas gerontology mostly targets things that are merely associated with age-related decline. For example, “longer lived animals express more sirtuins, let’s try supplementing humans with sirtuins and see what happens”.
Another problem with the gerontology approach is that assessing its efficacy is really difficult. Since damage repair aims to rapidly reverse the accumulation of damage, you can expect to observe the removal of damage, improvement of ageing biomarkers (more on these later), and hopefully some gain of function shortly after the therapy is administered, if it works. Gerontology, on the other hand, only aims to moderately slow the progress of ageing, so no matter how you measure that progress, it’s going to be years before you can confirm that effect in humans.
Indeed, this is part of the reason why most evidence for gerontology approaches is in mice. Calorie restriction can extend lifespan by up to 40% in mice, which is easy to measure since they only live about 2 years naturally. Unfortunately, it seems unlikely that any such approach could yield a comparable proportionate life extension in humans. We would have discovered a very long time ago if starvation could extend human lifespan by 40%, and there is little reason to believe that drugs that trick the body into thinking it’s being starved could do much better (resveratrol, metformin, rapamycin).
Calorie restriction is definitely good for you, as are exercise and sleep, and by all means, experiment with supplements to optimise your own health as much as possible. Even if it only extends your life by a couple of years, that might be the difference between living long enough to live forever and dying just before genuine rejuvenation therapies arrive. But in the long run, slowing the ageing process is only kicking the can down the road, and it is only rejuvenation, synonymous with the reversal of damage, that can truly rescue us from ageing. Gerontology is neither rejuvenation nor a stepping stone towards it, despite its humbler aspirations. Rejuvenation is harder, but it is doable, and the return on investment will be immeasurably higher.
Stop treating disease, start fixing damage
Our current paradigm for treating age related disease generally revolves around finding a single small molecule, that binds to a single target, inhibiting a single pathway, to treat a single disease. It’s like we see disease as a state in which the body is doing something bad, so we try to treat disease by stopping the body from doing what it’s doing. That modern healthcare has earned the moniker “sickcare” gives you some idea of how effective this has been.
Previously I had accepted that our mediocre results against chronic illness were reflective of the overwhelming complexity of biology, that biomedicine was just a ridiculously hard problem, and our best chance was to keep pouring billions into the pharmaceutical industry while hoping that advances in AI would make the complexity tractable. When viewed through a damage repair lens however, it suddenly seems a lot more obvious that this whole approach is doomed no matter what resources we throw at it.
Function follows form; these things we call diseases are functional consequences of damage, and if you don’t repair that damage then it will continue to accumulate, faster and faster as damage causes more damage, including to the body’s own damage repair systems, and eventually the damage overwhelms you no matter what else you do. Even if you succeed in mitigating the effects of current damage, it will just accumulate further until it causes yet more problems that you can’t mitigate.
Not only that, but the whole concept of “disease” is somewhat arbitrary. What exactly is a disease anyway? Sometimes it’s unclear to me whether disease refers to a set of symptoms or a cause of symptoms. Wikipedia defines disease as “a particular abnormal condition that negatively affects the structure or function of all or part of an organism, and that is not immediately due to any external injury”. The word “condition” is vague, and could refer to cause or symptoms, likewise, degraded structure means cause while degraded function means symptoms. Furthermore, the pathologies of age don’t always fall neatly into distinct buckets; often there’s a continuum of dysfunction with no clear boundary between one disease and the next. Anyone who’s presented symptoms that a doctor struggles to classify knows what I’m talking about—sometimes there simply is no diagnosis that cleanly captures a patient’s symptoms.
With infectious diseases, there is a mostly one-to-many mapping between pathogens and the symptoms they cause. Thinking in terms of disease makes sense when dealing with infection: a guy has a particular kind of cough, it’s caused by this particular pathogen, and we can kill it with this particular antibiotic. The disease name can refer to both the symptoms and the pathogen together, since they go hand in hand. Indeed, I find it telling that Wikipedia’s Disease page leads with a picture of some Mycobacterium tuberculosis. I think our usage of the word “disease” in relation to chronic illnesses is a holdover from our approach to infectious disease. We’re good at treating infectious diseases, and instinctively we’ve applied the same thinking to chronic illnesses, but it hasn’t worked. It’s worked so badly that age related sickness continues to kill literally everyone who doesn’t die of something else first.
One reason it doesn’t work is that the relation between causes and symptoms is much more complex in the case of ageing than with infectious disease. Infections generally occur separately, and the causative pathogens are usually easy to identify from symptoms and verify by testing. When we say we’ve diagnosed an infectious disease, we mean we’ve identified the pathogen that caused the symptoms, and thus the treatment is known. Age related diseases on the other hand are typically more like syndromes, collections of symptoms whose root cause is poorly understood. This is because unlike infectious diseases, age related diseases have multiple causes which occur all at once, each of them causing multiple downstream problems which interact with each other in complex ways. The relationship between causes and symptoms is therefore many-to-many rather than one-to-many, with each damage type ultimately contributing to multiple overlapping downstream pathologies, so there isn’t always a single type of damage that drives a particular illness. This is even more true when you consider that damage types can cause each other, whilst also damaging the systems that would normally repair them—this is why health declines exponentially in old age. In short, the chains of causality linking damage to pathology are long and tangled, that’s why isolating a pathology is rarely useful with regards to treatment.
By contrast, focusing on damage rather than pathology bypasses this complexity by recognising that we don’t need to unravel the mechanisms by which damage causes pathology, nor the mechanisms by which damage is created in the first place. We know that all age-related pathology is ultimately caused by some kind of damage, and we have a pretty good idea of the form and nature of that damage—indeed, we haven’t discovered a whole new type of age-related damage since the 1980s, which strongly suggests that our current catalogue is comprehensive.
If, in the course of debugging your code, you find something that is obviously a mistake, then it is wise to fix it immediately, whether or not you understand how that bug might be causing your program to misbehave. Personally, I do like to spend time picking those mechanisms apart until I understand them entirely, and I think that’s good practice for engineers who are building systems. But in biology, we are not building our own system, so we do not have the option of keeping it well documented and well understood. Instead, we are presented with an ungodly mess of uncommented spaghetti code, an enormously complex system that we did not ourselves design, but must still debug.
Another problem with thinking in terms of disease is that we generally don’t consider our symptoms to be a disease until they reach some arbitrary threshold of pain and dysfunction at which they seriously interfere with our lives. Think of all those sub-clinical aches and pains that you’re probably growing accustomed to if you’re above the age of 30. These pains are as much a manifestation of ageing as is Alzheimer’s disease, and just like Alzheimer’s, they must be caused by some form of damage. Why else does your neck hurt when you’re 45 but not when you’re 25? Something in your body must have changed to have caused that, and the solution is to revert that change. Why wait until you can no longer sleep before getting it fixed? Probably because most of our current treatments have such unfavorable risk/benefit ratios that it’s hardly worth trying them until you are quite desperate.
This brings me to another massive advantage of damage repair over disease treatment. Directly modifying the body’s structure like a mechanic fixing a car may sound dangerously gung-ho, since we clearly don’t understand the system we’re meddling with. It may sound like it would be safer to only interfere with processes whose immediate role in disease is well understood, but it’s actually the other way round. Most modern pharmaceutical products work by inhibiting the function of some receptor, signalling molecule, enzyme, gene or biochemical pathway, usually for the long term (since, you know, it won’t actually cure you—that’s why they’re called chronic illnesses). The problem is, we’re supposed to have those things. Whatever biomolecule you target will generally have at least one important role somewhere else in the body, probably more like 50 roles since this is biology. Damage, on the other hand, is defined in such a way that it’s definitely not supposed to be there. You’re not supposed to have senescent cells everywhere, your lysosomes are not supposed to be clogged with lipofuscin, your proteins are not supposed to be gummed together by advanced glycation end products, we know this because a) we can clearly see how these things impair function and b) they are absent in healthy youthful bodies that work correctly.
The damage repair therapies themselves may put transient stress on the body (e.g. cellular debris from the destruction of senescent cells may cause inflammation until it is cleared up by macrophages), and we may screw up and produce off-target effects (e.g. killing innocent cells, accidental interactions with non-target molecules). But the point is that we don’t have to worry about side-effects from on-target effects. Not only that, but most repair therapies under consideration today remove whole chunks of damage all at once, and it takes decades for damage to re-accumulate, meaning repair therapies can be applied in a “hit-and-run” fashion rather than constantly. This is intrinsically much safer.
Instead of trying and failing to treat age-related diseases one by one, we can slow, prevent and alleviate one or more age-related syndromes at once by intervening in fundamental ageing processes[1]. This way of thinking has acquired a name: the Geroscience Hypothesis[2][3]. It’s a little broader than the damage repair framework since it includes slowing the accumulation of damage as well as repairing it, but the idea that the best way to cure age-related disease is by intervening further upstream in ageing itself is spot on.
It would be very nice if the FDA could be made to understand all this. Right now, nearly all longevity trials are required to have some specific disease as their primary endpoint, even though the interventions they’re testing often improve health and resiliency generally.
To progress more rapidly, we need to be allowed to evaluate and ultimately prescribe drugs specifically for the purpose of repairing damage. The alternative is to allow stuff that is unambiguously bad for you to progress and accumulate, refusing to remove it until it causes symptoms, which you may struggle to connect to that damage. Although it goes without saying that doctors must weigh the benefits of treatment against the risks (which are intrinsically high for novel treatments), allowing damage to progress risks causing secondary damage that we might not know how to fix, or even know exists.
There is some sign of movement on this front: a recently funded trial to test the lifespan boosting effects of the anti-diabetic drug metformin has created a new FDA-approved endpoint that represents ageing in all but name[4]. Instead of measuring the severity of some particular disease, it’s a composite metric tracking multiple biomarkers of general function. The hope is that once this trial progresses, other companies will feel confident using the same endpoint for their own products.
Primary damage, secondary damage
I’ve defined damage as “any structural change that causes a loss of function”, with causality understood in the Judea Pearl sense of “that which would make a difference if we were to change it”. But ageing bodies show changes in just about all aspects of structure, so how do we know which are causative, in the sense that reversing them would cause function to improve? We could of course proceed empirically, targeting different structural alterations in turn to discover which ones have an impact on function. But that leaves us with a lot of targets to work through.
My understanding is that the SENS platform cuts this workload down by emphasising primary damage as the rational target for intervention. Primary damage is that which is created as a direct side-effect of ordinary metabolism. This is a matter of identifying the root causes of disease—which is arguably what medical science is all about. Age-related diseases are caused by age-related structural changes, and although age-related structural changes cause each other in complex networks, they can all ultimately be traced back to ordinary metabolic processes—that’s why these changes eventually affect everybody, regardless of lifestyle. By targeting primary damage, we trace the etiology of disease as far upstream as possible without trespassing into metabolism.
Atheromatous plaques, macular edema, stooped posture and cell membrane stiffening are all examples of secondary damage that exist downstream of the primary damage listed in the SENS platform. Fixing the SENS damage types should prevent them from occurring, but won’t necessarily fix them if they’re already there. Some of them might fix themselves once the primary damage is fixed, others might require separate interventions in those individuals old enough to have already acquired them before we can fix the primary damage that causes them.
AGI, Nanotechnology
We do not need to wait for AGI nor molecular nanotechnology to solve this problem for us. I may be wrong here, but I get the impression that people in the transhumanist/rationalist space sometimes have the mindset that ageing is such an intractable problem that it isn’t even worth trying to unravel it with our pitiful human meat-brains, to the point where it would be easier to just invent God first and then get God to do it for us. The problem is that a) we don’t know how to do that and b) it’d be super dangerous if we did, but we do now have plausible plans for repairing damage.
I liken it to SpaceX’s plans for Mars colonisation: we don’t need any major scientific breakthroughs to make it happen, we just need to overcome a lot of engineering problems, and humans are good at those. Elon isn’t betting on miniaturised fusion power or aerospike nozzles or esoteric ultra-high-performance materials, he thinks we can get to Mars using relatively conventional technology, and there’s no obvious reason why his plan shouldn’t work. I think that’s where we are with ageing right now. We know that all loss of function is caused by damage of some kind, we know what are the main types of structural decay that drive ageing, we haven’t discovered a totally new one since the 1980s, and there exist plausible strategies for the elimination or obviation of all of them.
As for molecular nanotech, I will note that a) manipulating matter at the atomic scale in a foundry is not the same as manipulating atoms in the body, and b) we already have nanobots, they’re called cells. The biotech sector is the real life nanotech sector. Cells are pre-existing nanobots, and they’re already perfectly adapted for getting shit done inside a living body. Sure, somewhere in design space there must exist nanobots that could do a more effective job of building and maintaining the body than cells do, but even with perfect nano-scale manufacturing tech, the difficulty of designing nanobots to do what cells do would be enormous. We should just use the cells.
Why do we age?
Wrong question. Ageing is primarily a phenomenon of physics; all machines do damage to themselves, so the real question is why do we live as long as we do, and why are there some species that don’t appear to age at all? The answer is that evolution has equipped us with damage repair systems of our own, and these keep us alive far longer than we would survive for otherwise.
An example: ordinary metabolism produces lots of waste products, and the body has to break them down or eliminate them or else they’ll build up until they kill you. For lysosomal storage disease patients, whose waste degrading enzymes are broken by a mutation, that’s exactly what happens, and they tend to die young.
The reason humans didn’t evolve to live even longer than we do is that life in the ancestral environment was rough, and so a mutation that extended health into later life would have no actual effect on most people, since they’d generally starve, freeze, die of infection or be killed before the age of 40 anyway. And if that mutation cost even a little bit of extra energy to run the damage repair machinery during youth, then it could confer negative fitness and be actively selected against.
Ageing Clocks
Ageing clocks are a rapidly growing field aiming to quantify ageing, so that we can quickly assess how effective an intervention has been at reversing or postponing it. It’s long term outcomes that we ultimately care about (how long before the patient gets sick, how long before they die), but we have to do a lot of waiting to measure those things directly, and time is of the essence. Ageing clocks allow us to predict those outcomes from biomarkers that we can measure shortly after treatment. The approach was pioneered by Steve Horvath[5], who built a regression model that predicts chronological age from DNA methylation state. This prediction is what the term “epigenetic age” refers to. Predictions of chronological age from biomarkers more generally are called “biological age”. If a person’s biological age is significantly lower than their chronological age then we can say that they’ve “aged well”, although “aged more slowly” would be more accurate. It’s not fundamentally different to guessing a person’s age by looking at their face, and using that as a proxy for their overall health—the difference is that we’re using molecular biomarkers as input instead of faces, and it’s done by a machine, so it’s consistent.
This approach is perfectly valid, because chronological age correlates so well overall damage levels and remaining healthspan in today’s world that they both make excellent surrogates of each other, so predicting chronological age pretty much means predicting damage levels and remaining life. Saying “he looks like a 30 year old” is the same as saying “he looks pretty healthy”. Health is the absence of damage and ageing is the accumulation of damage, so estimating greater age means estimating greater damage and lower health. I do feel the term “ageing clock” is a little misleading, though. It implies that there’s a single hidden process that drives and orchestrates the functional decline we call ageing, that the body holds within it a secret number called “biological age” which ticks up regularly, that we can read it with a regression model, and perhaps that we could even edit this one thing directly, and thus sidestep all the divide-and-conquer damage repair stuff by just telling the body to be younger. Maybe I’m reading into it too much. To be abundantly clear, I’m not saying that ageing clocks themselves are bad—it’s super important that we have a way to measure how healthy people’s bodies are. I just think they’re badly named.
More recent ageing clocks such as GrimAge[6] have been trained to estimate remaining healthspan directly, rather than using chronological age as a surrogate. This may prove to be more useful. The worry with training to estimate age rather than healthspan is that there may be “superficial” biomarkers, which reliably change with age but cannot be said to cause ageing, in the sense that reverting them does not restore function because they were mere side-effects of whatever it is that really does matter. An age regression model would learn to use these markers, and would thus predict lower biological age after a therapy that reverted them, even though they don’t really predict a better outcome. A model trained explicitly to predict the things we actually care about would presumably be less susceptible to such a failure mode.
Examples
This essay focuses on conceptual shifts, but I need to emphasize that this is not just a cool way of thinking—these ideas are being put into practice in laboratories right now, and they are yielding results. Here I describe four damage repair therapies currently in development, which illustrate the principles outlined above.
Senolytics
Senescent cells are a type of bad cell that accumulates with age. Often referred to as “zombie cells”, they have lost the ability to divide, but that’s not what makes them actively dangerous. Senescent cells are relevant to ageing because a significant fraction of them produce senescence associated secretory phenotype (SASP), a witch’s brew of inflammatory cytokines, proteolytic enzymes, fucked up lipids and growth factors[7]. SASP plays a key role in driving inflammageing, the systemic, chronic, sterile inflammation that develops slowly with age and is widely understood to be bad for you[8]. Senescent cells accumulate at the pathologic sites of many age-related disorders including osteoarthritis, atherosclerosis, Alzheimer’s and macular degeneration, and bad things seem to happen to mice when we inject them with more of them. SASP can also cause other cells to become senescent, which partly explains how their numbers increase exponentially in old age. So we have these broken cells who proliferate in the elderly and look like they’re causing trouble: sounds like a great example of an age-related structural change that causes a loss of function, i.e. damage.
Cellular senescence probably evolved primarily as an anti-cancer mechanism. Cells can become senescent in response to a wide variety of stressors[9], particularly those which involve DNA damage, suggesting that senescence preserves function by preventing the replication of damaged DNA. The prototypical form of cellular senescence is replicative senescence, discovered by Leonard Hayflick in 1961[10], in which cells cease to divide after a certain number of generations due to the depletion of telomeres (little end-caps on chromosomes). Every time a cell divides, the daughter cells will have shorter telomeres; when they run out, the ends of chromosomes start to fuse and the cell becomes senescent. The Hayflick Limit, as it has become known, can be thought of as a last line of defense against cancer, kind of like a recursion depth limit: any would-be tumour that does not figure out a way to lengthen its telomeres will inevitably hit the Hayflick limit, become senescent and cease to grow, leaving you with a mole or skin tag instead of a tumour.
Preventing cells from becoming senescent, or reversing their senescent state, may therefore be a bad idea, but what we can do is remove them. Since they are relatively few in number, killing them and allowing them to be replaced by the division of healthy cells is a perfectly viable strategy for repairing the damage that they constitute. Fortunately this turns out to be surprisingly easy, with several repurposed FDA-approved anti-cancer drugs showing senolytic action. Progress in developing senolytic therapies has therefore been gratifyingly rapid, with several clinical trials currently in progress. Given that SASP was only discovered in 2008[11], this is remarkably fast by typical drug discovery standards. Senolytic drugs are therefore arguably the tip of the spear in the quest for bona-fide rejuvenation therapies.
These clinical trials are very well motivated by studies in rodents. Senolytic drugs have been found to restore cognitive ability by improving neurovascular function[12] and reducing brain inflammation[13], alleviate obesity-induced anxiety[14], restore muscle hypertrophy[15], and extend median lifespan[16]. A first-in-human trial of the first senolytic therapy, dasatinib + quercetin, significantly improved physical function in idiopathic pulmonary fibrosis patients while being well tolerated[17], and a later trial confirmed that it reduced markers of cellular senescence in diabetic kidney disease patients[18]. Senolytic therapies are also being pursued by multiple private companies, notably Unity Biotechnology and Oisin Biotechnologies.
One theme that emerges from this body of work is that rather than being cleanly associated with certain diseases, senescent cells are broad-spectrum disruptors of health generally, contributing to many if not most age-related chronic diseases along with more nebulous afflictions such as frailty and loss of gait speed[3]. Hickson et al.: “If senolytic agents can be shown to be effective for several individual age-related conditions, they may prove to have a role beyond alleviating single diseases: they may be effective in reducing the multimorbidity common in elderly patients”[18]. Stop treating disease, start fixing damage.
LysoClear
Age-related macular degeneration (AMD) is a leading cause of central blindness among the elderly population worldwide[19]. It is caused by an accumulation of intra-cellular waste, notably a substance called A2E, which is produced as a by-product of the high-energy photochemistry which transduces incoming photons into neural impulses in retinal rod and cone cells. Humans do not possess enzymes capable of degrading A2E, so it ends up slowly accumulating in pigmented retinal endothelial (RPE) cells, which form the posterior lining of the retina. The dose makes the poison, and so at some point, A2E reaches sufficient concentration that it begins to kill RPE cells, which is unfortunate because RPE cells are essential for the survival of rods and cones. The result is a progressive loss of central vision, right where the density of rods and cones is greatest.
Standard of care for AMD consists of vitamin supplements[20]. These can moderately slow the progress of AMD, but they cannot stop it, nor reverse it. In the more advanced and serious “wet” form of AMD, in which new capillaries grow into the retina, leak plasma and cause macular edema leading to legal blindness, we prescribe VEGF (vascular endothelial growth factor) inhibitors. VEGF inhibitors are very effective at preventing catastrophic vision loss and even restoring some function in wet AMD, but they are not without side-effects[21]. VEGF is an important signalling molecule that we are supposed to have, which plays a multitude of roles throughout the body, so it’s not surprising that knocking it out has its risks.
It’s well established that A2E plays a causative role in AMD, it’s definitely not good for you, and young people don’t have a lot of it. What if instead of trying to inhibit AMD’s pathological processes with supplements and angiogenesis inhibitors, we targeted the root cause of AMD by removing A2E from the body directly? I don’t mean to imply that prior researchers had been stupid here; humans don’t come equipped with enzymes capable of degrading A2E so it wasn’t exactly obvious how to get rid of it. It took the pioneering work of the SENS Research Foundation to discover a bacterial enzyme that could do the job through something akin to bioremediation; this work was later spun out into LysoClear and pursued by Ichor Life Sciences. LysoClear is currently undergoing pre-clinical trials in vivo[22], and has produced encouraging results so far[23].
Thymus Regrowth
The thymus is a small lymphatic organ located behind the breastbone. It is the site at which T-cells mature (hence the name), and where they undergo a filtering process that kills T-cells that see host proteins as foreign or that respond to “naked” antigens, which are not presented by other immune cells. The thymus is an unusual organ in that it recedes (or “involutes”) early in life, beginning at infancy and having become mostly replaced by fat tissue by adulthood. Without the thymus, the body is unable to produce new naive T-cells, and this is thought to play a role in both the decline in resistance to infection and the rise in carcinogenesis with age[24]. Why would such a loss of function evolve? It may be an example of antagonistic pleiotropy, by which an organism may trade long-term self-maintenance for short-term survivability. Thymic T-cell production is energy intensive, and the T-cells produced early in life seem to last pretty well until old age, so it has been suggested that thymic involution may enhance reproductive fitness early in life, while its cost is not borne until late life, by which time most people in the ancestral environment were dead anyway[25].
Greg Fahy is the pioneer of vitrification for organ and tissue cryopreservation (which naturally is also state-of-the-art for whole body cryopreservation in cryonics). These days, he works on regrowing the thymus. Turns out this is way easier than you’d think—you don’t need stem cells or bioprinting, it can be done to an impressive degree just with small molecules, namely with a combination of human growth hormone, DHEA and metformin[26]. The hGH makes the thymus regrow, and DHEA and metformin are diabetes medications that counteract the excessive insulin production caused by hGH. The original trial was quite small, so an extended and improved re-run is currently in progress, which so far is replicating the original results[27].
This particular example is still very preliminary, but I find it compelling because this one intervention appears to reverse multiple age-related changes in humans, not all of which are obviously related to immune function. Improvements measured by Fahy’s team include not only confirmed regrowth of the thymus and bolstering of naive T-cell populations, but also a reduction in cancer risk factors and systemic inflammatory markers, improved kidney filtration rate, and improved prostate health. Also a guy’s hair apparently grew darker again. This probably isn’t entirely due to thymic regrowth, since hGH, DHEA and metformin are all known to have anti-ageing properties of their own, and there’s certainly some synergy between them.
It also illustrates that “damage” does not necessarily mean “wear-and-tear”—thymic involution in particular appears to be very much a regulated change and a part of the developmental program. But damage is defined here as any structural change that causes a loss of function, regardless of how it came to be. It doesn’t ultimately matter how the thymus involutes nor why, in the proximal or evolutionary sense—we just want our T-cells back.
Another significant outcome from hGH + DHEA + metformin is the first-in-human reversal of epigenetic age, according to four different ageing clocks[26]. Patients’ epigenetic ages were on average 1.5 years younger at the end of treatment, which lasted for one year, than they were at the start, meaning their biological age was 2.5 years younger at the end of treatment than it would have been naturally. This is important because epigenetic clocks are standardised, so they don’t allow the authors to cherry-pick markers that tell a positive story. This is strong evidence of a broad-spectrum rejuvenation effect—exactly what you would expect when you fix a key system that’s obviously broken.
Source: Reversal of epigenetic aging and immunosenescent trends in humans
Curing Atherosclerosis
Cardiovascular disease, driven principally by atherosclerosis, is the leading cause of death globally[28]. Briefly: cholesterol gets stuck in your artery walls, macrophages come to clean it up, it poisons them and they die, more macrophages come to eat the dead macrophages and they die too, and after several decades of this you end up with an atheromatous plaque: a grossly visible accumulation of dead macrophages and pools of extra-cellular cholesterol. Eventually the plaque ruptures, spewing debris into your arteries, blocking them and causing you to die. This process begins in youth, and will eventually kill everyone who doesn’t die of something else first, regardless of lifestyle.
The state-of-the-art treatment for cardiovascular disease is statins, which moderately slow the growth of atheromatous plaques by reducing the amount of cholesterol-carrying LDL exported by the liver. Statins have side effects that make them unusable by some patients, for which reason they are rarely prescribed until a plaque has been confirmed, by which point its progression is typically quite advanced, and they do nothing to reverse the growth of that plaque. Can damage repair do better? Instead of slowing the plaque’s growth or learning to live with it, can we remove it directly? Here there are not one but two commercial enterprises pursuing promising damage repair approaches: Repair Biotechnologies (founded by Reason, the guy from fightaging.org), and Cyclarity Therapeutics.
Repair are developing a cell therapy consisting of macrophages enhanced with their proprietary Cholesterol Degrading Platform (CDP). CDP enabled cells are able to degrade seemingly limitless amounts of cholesterol internally, and so do not succumb when doused with the stuff. Furthermore, these macrophages are derived from allogeneic “off-the-shelf” stem cells that have had their immune markers stripped from them—this makes the whole process considerably cheaper and more streamlined than extracting, modifying and re-injecting the patient’s own macrophages.
Source: Repair Biotechnologies
Armed with upgraded cholesterol processing ability, CDP-enabled macrophages are able to do the job that regular macrophages fail so catastrophically at: inject them into a mouse with atherosclerosis and they dive into the plaque and eat it, shrinking its size substantially as they break the cholesterol down into harmless metabolites.
Meanwhile, Cyclarity (formerly Underdog Pharmaceuticals) are pursuing a small molecule approach that removes 7-keto-cholesterol (7KC) from cell membranes. 7KC is a form of oxidized cholesterol produced by reaction with an oxygen radical. Unlike regular cholesterol it is straight up toxic and has no known physiological function, but it does play a role in many age related diseases, not just atherosclerosis[29]. It’s a great example of a single type of damage that plays a role in many age-related disorders (check the review article I cite, it’s really a lot). Like A2E, 7KC is a toxic byproduct of normal metabolism that accumulates slowly enough that most humans in the ancestral environment were already dead before it became a problem, therefore evolution never got around to clearing it up. If cholesterol is bad for macrophages in excess, 7KC is just bad full stop.
Cyclodextrins are soluble, macrocyclic carbohydrates that can thread themselves around a small hydrophobic molecule like cholesterol and bind to it, then float off into solution with it. Cyclarity’s approach uses rationally designed cyclodextrins with high affinity and specificity for 7KC to remove it from cell membranes[30][31]. They are non-toxic and are excreted from the body via the kidneys, which is ultimately how they remove 7KC from the body.
Combination Therapy
Damage repair therapies have so far elicited only modest lifespan extension in mice. It’s impressive, but if it’s such a great idea then why hasn’t it yielded serious lifespan extension yet?
The problem is that damage takes many different forms, and any one of them can kill you if it gets bad enough. Not only that, but they accumulate at such a rate that they’ll all kill you at around about the same age. How could such a coincidence occur? Recall that long lived species like ourselves live long because they have evolved to repair damage. But there’s no point in repairing different types of damage at different rates (that is, such that they become problematic at different ages). If you do that, then your lifespan will be limited by whichever type of damage kills you first, and your stronger ability to repair all the other types will be wasted. In this situation, there is no selection pressure to maintain the repair capacity of any except the fastest accumulating damage type, because mutants who repair other damage types more slowly will live no shorter lives. If damage type X kills an organism at 20 years of age but damage type Y would only be a problem if it lived to 50, then a mutant who repairs Y more slowly, such that it becomes lethal at 40, would still die at 20 due to X. Without selection pressure to maintain them, random mutations will degrade excessively efficient repair systems until all forms of damage become relevant at the same age. And if you save energy or nutrients by repairing Y more slowly, then that’s a fitness increase and will be actively selected for.
With this in mind, it is not surprising that senolytics cause only modest lifespan extension in mice. It’s surprising that they are able to extend lifespan at all. The fact that they do, probably implies that senescent cells have a deleterious effect on the repair of several other forms of damage, such that they all accumulate a little bit slower when senescent cells are cleared. But the real extension of healthspan will come when we repair multiple forms of damage at once.
Epigenetic reprogramming
In 2006, Shinya Yamanaka’s lab discovered that a group of four transcription factors known as OSKM (oct-4, sox2, klf-4 and c-myc) are sufficient to transform ordinary somatic cells into induced pluripotent stem cells (iPSCs). PSCs are able to proliferate indefinitely without hitting the Hayflick limit (they express telomerase, which lengthens their telomeres) and can differentiate into any somatic cell type, so naturally they’re pretty relevant to regenerative medicine. Since cells generally become more differentiated and less stem-like as an organism develops, transforming adult somatic cells back into iPSCs could be thought of as a reversal of developmental age.
As I understand it, the usefulness of epigenetic reprogramming is twofold: it can reverse the accumulation of epigenetic noise which has been proposed as a key driver of ageing[32], and it can effectively create new stem cells in the body, which is potentially more elegant and easier to implement than injecting stem cells.
The concept of regeneration has been perhaps conspicuously absent in this post so far, but here is a good place to mention it. You may know that there are some animals such as salamanders, hydra, and planarian flatworms, who are capable of regenerating whole limbs and other complex structures including brains following injury or amputation. Turns out mammals can do this too, but the ability becomes incrementally suppressed following the embryonic fetal transition (EFT, about 8 weeks post fertilization in humans)[33]. Prior to the EFT, you can grossly mutilate an embryo (at least a mouse embryo, I don’t think it’s been done with humans) and it will regrow the lost tissue perfectly with no scarring.
This is clearly a very important form of innate damage repair, since we have little idea how to manually reconstruct lost or damaged tissues. Organ bio-printing is a thing, but the masters of tissue assemblage and repair are cells themselves—it is their art that we imitate with bio-printing, and we can expect superior results if we can coax them into doing the job for us. Adult mammals of course can already heal from wounds, which is a form of regeneration, but it’s limited, it involves scarring, and they cannot regrow limbs or organs that are amputated. But if we get reprogramming right, we could potentially heal from greater harms—for example, application of OSK has been shown to regenerate crushed optic nerves in mice[34].
The suppression of regeneration post-EFT probably evolved as an anti-cancer mechanism (although this view is disputed), since stem cells are cancer-like in many ways: both can replicate indefinitely, both show a metabolic shift toward aerobic glycolysis, and they both express similar genes that are suppressed in normal adult somatic cells. As such, we need to be careful when reverting cells to this state via partial reprogramming, and indeed it’s been found that if you rewind the developmental clock too far, cancer happens[35].
Epigenetic reprogramming seemed to me like a competing approach to damage repair for a while, but now I just see it as a type of damage repair. In terms of the SENS platform, it’s an alternative approach to stem cell therapy for fixing cell loss, since it can enable cells to proliferate free from telomeric restriction in order to repair and replenish damaged tissues—kind of like creating stem cells inside the body. It may also turn out that random changes to the epigenome itself constitute an 8th category of damage in their own right—the questions are a) how much does it impact function, and b) how much might it normalise itself if we fix all the other things that stress cells out? We’ll probably have to find out empirically: try many combinations of damage repair therapies including epigenetic reprogramming to find the minimal, safest combination that yields the greatest improvement in function.
What is clear is that partial epigenetic reprogramming won’t be enough on its own. There are too many other things going catastrophically wrong in the ageing body for me to believe that reprogramming could fix everything. What about all the junk accumulating because we lack the genes to code for enzymes that can break it down? Epigenetic change cannot make a cell express genes it doesn’t have, so we’ll have to deliver either the enzymes or genes for the enzymes. How will reprogramming reduce atheromatous plaques, how will it remove advanced glycation end-products, how will it regrow the thymus? SENS Research Foundation have a piece here making the same argument in much greater detail.
The results that excite me the most in reprogramming are regeneration-focused papers like this one, in which the optic nerves of mice were crushed and then regenerated by application of OSK (although the effects were diminished in older mice). One might argue that the SENS platform somewhat sweeps that kind of damage under the rug of “cell loss”, which to me seems like too limited a description. It’s not just the number of cells that must be restored, but the way they are organised relative to each other spatially; the magic of stem cells is not just that they replace lost cells, but that they know where to go, what to do and how to form functional networks once they’re there. It’s morphology that we’re restoring, not just numbers, and that requires us to invoke the magic of regeneration because we have no idea at all how to do something like manually repairing a crushed optic nerve at the cellular level.
The results from most other reprogramming studies don’t seem super exciting so far[36]. I see a lot of papers reporting reprogrammed cells that “look more youthful” in terms of their epigenetic, transcriptional and secretory profiles, but fewer that claim to restore actual function. Mouse lifespan has been marginally extended, but so far only in progeroid mice. A frequently reported endpoint seems to be reversal of epigenetic age, which is not super surprising given that the intervention is twisting the hands of the epigenetic clock directly. Epigenetic changes correlate with age (hence epigenetic clocks), but that doesn’t mean they’re a cause of ageing—cells may well be switching genes off and on as they adapt to the increasingly stressful environment they’re in due to other age-related changes. In that case, epigenetic reprogramming would be a bit like preventing rain by twisting the needle on a barometer—and then citing the barometer as evidence of weather control. This is consistent with the fact that thymic regrowth reduces epigenetic age without direct epigenetic reprogramming, and also with the fact that many studies showing reprogrammed cells acting more youthful are in vitro, meaning they’ve been taken out of the inflammatory environment of an aged body.
Regeneration is still quite mysterious (or rather, our understanding of it sucks), therefore regenerative medicine still feels a bit like voodoo. Much of reprogramming so far seems to boil down to dosing mice with different reprogramming factors with different time schedules and hoping for the best. In contrast, the SENS platform emphasises combination therapies that remove things that are definitely not meant to be there and are almost certainly harmful. I get more excited about the various SENS branches because they have simpler and more direct rationales as to why they should improve function. Call me short-termist, but I get more excited by things that we can do right now and expect results.
Morbidity compression
The widespread belief that the diseases of ageing and ageing itself are separate things has led to the idea that people will “die healthy” in their old age, once the cruel and debilitating diseases of ageing have been cured. Ageing itself, it is thought, is a benign and gentle killer, waiting to whisk us away one night once our allotted time on Earth is up. Bullshit, says I. People don’t die because they get old, they die because they get sick. The boundaries between ageing and age-related disease are arbitrary; it is not possible to cleanly separate them, nor is it possible to cure age-related diseases without reversing the accumulation of damage, i.e. rejuvenating people. We have a choice: either rejuvenate, or make our peace with Alzheimer’s disease, macular degeneration, strokes, cancer, cardiovascular disease, osteoarthritis, and all the other diseases of age that we currently spend billions fighting every year.
The easiest way to achieve morbidity compression would be to pursue total rejuvenation through damage repair as outlined above, live your life as fully as possible in a state of perfect health for 500 years, and then die by hitting a tree while skiing down everest. Alternatively, if 500 years sounds too long, we could implant all rejuvenation patients with a device that stops their hearts at some random time around the age of 80. If dying healthy at age 80 is what society truly desires, then I’m sure it will have no problem implementing this solution.
Longevity Escape Velocity
A note about longevity escape velocity (LEV) is appropriate at this point. The idea is basically that early rejuvenation therapies will buy you time in which the therapies can be improved further, thus allowing you to extend your deadline even further by the time that deadline arrives, and so on and so on. Not only that, but the deadline extends by a greater amount with each incremental improvement, because each time there will be fewer and fewer types of damage that we don’t know how to control. LEV, then, is the rate of technological progress that, on average, extends your remaining life expectancy by more than one year per year. The upshot of this is that age-related mortality will become a thing of the past long before we are able repair damage comprehensively.
I find it a somewhat slippery concept to define precisely, but it boils down to this: people will stop dying of ageing before we have the technology to comprehensively rejuvenate them, because partial rejuvenation buys time in which to improve the tech further. LEV is the point at which people no longer die of ageing, and it comes before the arrival of comprehensive damage repair.
I said before that there are types of damage, each of which can kill you all by itself at around about the same age. However, within these types there are generally subtypes, which have an additive effect on the impairment of function. For example, there are thought to be many subpopulations of senescent cells in humans, each of them impairing tissue function in more or less the same way but requiring different interventions to remove them. If you can clear half of these senescent cell types then it’ll take twice as long for the remaining ones to accumulate to levels that cause the same amount of trouble (assuming they each accumulate at the same rate). That’s why incomplete damage repair can still extend lifespan, so long as some of the damage of each type can be repaired.
An important corollary of all this is that extending life expectancy from 150 to 1000 is much, much easier than going from 85 to 150. Let’s say we manage to boost life expectancy to 150 while the oldest generational cohort are about 120. Perhaps you’ve learned to repair about 50% of damage subtypes in each category, so the overall rate of ageing has halved. But to half the rate of ageing a second time, you only need to learn to fix the next 25% of damage—with the benefit of all the knowledge, experience and infrastructure you’ve already grown. Cracking the next 12.5% doubles life expectancy a third time. An easier way to see this perhaps is that—if you ignore non-age-related mortality—lifespan must asymptote toward infinity as we approach comprehensive damage repair. But the portfolio of damage we must fix is finite, so lifespan must extend faster and faster as we approach completion.
The War On Ageing
So how long before we stop dying? The problem with timeframes is that they depend on what people actually do, and that in turn depends on where money is invested. There is a sense in which timeframe predictions may be self-fulfilling: if people think LEV is near then they’re going to be more inclined to invest funds and careers in that direction. Your guess is as good as mine really, but intuitively, I feel like reaching LEV by 2040 is possible, if society commits to a full scale, government funded war on ageing. At some point, I think this will happen. We’re not going to suddenly stumble upon LEV with no idea it was about to happen—at some point, we will achieve laboratory results that make it undeniable that radical healthy life extension is feasible in humans.
Aubrey de Grey is currently pursuing such results full throttle at the Longevity Escape Velocity Foundation (LEVF), a longevity Manhattan Project aiming for such extreme life extension in mice that the achievability of LEV in humans becomes undeniable. Their goal is to extend the mean and maximum lifespans of mice that normally live to 30 months by at least 12 months, with interventions that are initiated no later than 18 months of age. Recently they acquired 1000 pre-aged mice, and will be testing various combinations of four interventions each of which have individually been established to extend mouse lifespan significantly. The experiment begins this month, January 2023. To the best of my knowledge this is the only combined therapy longevity study in existence, and it is funded entirely by philanthropy. Studies of this nature are very expensive, so if you want it to go faster, click here to throw money at LEVF.
Alternatively, it may turn out that early damage repair therapies in humans are able to catalyze the appropriate enthusiasm, particularly if they clearly reverse some aspect of what people call “ageing itself”, e.g. cognitive decline, reduced walking speed, grey hair, etc.. A lot of exciting stuff is in the pipeline[37][22], and optimism around genuine rejuvenation could snowball if even a fraction of these elicit a modest broad spectrum rejuvenation effect in humans.
It’s helpful to consider the COVID pandemic in this context. People in this community are well aware of the FDA’s “invisible graveyard” problem, whereby their incentives punish them far more severely for deaths caused by hastily approving a dangerous product than for deaths caused by failing to approve something safe and effective. Unless that product is a COVID therapy. When the pandemic hit, we adopted a sort of wartime mentality. The perceived threat from COVID was great enough that the public actually gained a sense of urgency, and sure enough, there was political pressure to approve certain therapies far faster than would normally be the case.
The infection fatality rate of SARS-CoV-2 is estimated at around 2%. The fatality rate of ageing is 100%.
However the War On Ageing begins, I think it’s going to feel a bit like when COVID hit, but crazier. People are going to wake up one morning and realize that they have a terminal but soon-to-be-curable illness. Ageing will transform in people’s minds, perhaps quite suddenly, from a depressing statistic that we all avoid thinking about to a screaming moral imperative. Longevity, or rejuvenation, or whatever name we settle on will come to dominate public discourse just as COVID did, the public will demand that rejuvenation therapies are funded and fast-tracked, every world government will have a plan of action to defeat ageing, and insane quantities of money will be unleashed—as is always the case in wartime. We will suddenly discover that we can move much faster than we thought we could.
Incidentally, there’s a good change that cryonics will finally gain acceptance and support once this happens. The difference between those who get cryonics and those who don’t is the anticipation of radical technological progress. Despite the entire history of humanity being defined by scientific and technological revolution, most people continue to believe that only slow, predictable, incremental progress is realistic, and that preserving people until we have the means to revive them is therefore delusional. This could change rather rapidly once society is frantically racing towards LEV, and a whole generational cohort realise that it’s not going to be quite fast enough to save them. Despite the utter contempt and ridicule reserved for cryonicists by the tiny fraction of society that acknowledges their existence, the field has made great strides over the decades, such that with a modest investment of actual funding, we could potentially save the lives of millions of people who would otherwise perish a few years before salvation arrives.
This is all happening sooner than you think. The concepts I’ve outlined in this essay are gaining traction rapidly; the idea that ageing is driven by accumulating damage that may be amenable to therapy has been pretty much accepted since The Hallmarks of Aging was published[38], meanwhile the idea that targeting fundamental ageing processes can delay, prevent and reverse multiple age-related disorders simultaneously has also gained traction[39][1]. Recently these ideas are even permeating into the corridors of power[40][41][42], and the popular media[43], and that’s to say nothing of the explosive growth in new companies and investment funding[44].
Conclusion
Motte: fundamental damage types that accumulate slowly in all humans are the root causes of age-related disease; multiple age-related diseases can be slowed, prevented and reversed simultaneously by targeting damage instead of the diseases themselves; several such therapies are already under development and could benefit humans within 5 years with sufficient focus, luck, and regulatory approval; ageing is not one thing, therefore combination therapies addressing multiple damage types will be necessary for serious lifespan extension.
Bailey: the SENS taxonomy of damage is comprehensive, i.e. all clinically relevant types of damage fall into one of its seven categories and are solvable by a plausible engineering approach already under development somewhere, fixing all of them will result in the indefinite extension of healthy life; an all-out, global War On Ageing is imminent; LEV could be be reached in a couple of decades (Aubrey’s prediction); most of us will look better at 100 than we do today.
There is a growing consensus that the processes we traditionally think of as “normal ageing” are in fact the root causes of the pathologies of late life, and that targeting these processes is the key to slowing, preventing and reversing age-related diseases. Ageing has traditionally been seen as off-limits to medicine, and that’s precisely why our progress against age-related disease has been so mediocre. This is finally starting to change: good shit is in the pipeline, with the first wave of bona-fide rejuvenation therapies making good progress and attitudes starting to shift in both academia and congress.
Rejuvenation is the sensible way to go about what we’ve been trying to do for decades, namely, curing the diseases of old age. Gerontology is no longer some esoteric field offering minor quality of life improvements in the elderly, rather, it’s going to be the lynchpin of modern medicine, and the single most important thing we can do to relieve pressure on health services. If we’re willing to spend billions researching a cure for Alzheimer’s, then we must focus that money on reversing the cellular and molecular damage that drives it (i.e. ageing), because that’s the only way to succeed. Medicine is supposed to save lives, and extending lives is the same thing—the stuff we call longevity biotech is just medicine that works.
In conclusion: fuck ageing, none of us signed up for this shit. It’s time to escape the Wheel of Samsara for real.
About me
My background is in computer vision and machine learning; here are some papers I published as a PhD / postdoc: https://scholar.google.com/citations?user=PJIQyL8AAAAJ&hl=en&oi=sra
I had the pleasure of attending both LessDeath (a sort of networking summer camp / workshop) and Longevity Summit Dublin (a conference) in 2022. A big part of why I did that was to get a sense for how widely embraced the damage repair paradigm is within the broader longevity movement, and hear some alternative viewpoints. I found some people objecting to specific technical points Aubrey has made, but damage repair itself seems to be pretty widely accepted. Both events were excellent and will be repeated at some point this year. It was at LessDeath that I met JackH, who posted Anti-Aging: State of the Art here two years ago. That was what inspired me to write a post of my own, but with emphasis on the specific concepts that have caused me to become optimistic about the feasibility and timeframe of LEV. There’s a lot of stuff I didn’t talk about here, so please ask me stuff in the comments if you have questions.
- ^
Aging: a common driver of chronic diseases and a target for novel interventions https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4852871/
- ^
What is Geroscience? https://www.afar.org/what-is-geroscience
- ^
The Clinical Potential of Senolytic Drugs https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5641223/
- ^
TAME: a genuinely good use of 75 million dollars https://www.researchgate.net/publication/336386513_TAME_a_genuinely_good_use_of_75_million_dollars
- ^
DNA methylation age of human tissues and cell types https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4015143/
- ^
DNA methylation GrimAge strongly predicts lifespan and healthspan https://pubmed.ncbi.nlm.nih.gov/30669119/
- ^
Cellular senescence and the senescent secretory phenotype: therapeutic opportunities https://pubmed.ncbi.nlm.nih.gov/23454759/
- ^
An Update on Inflamm-Aging: Mechanisms, Prevention, and Treatment https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4963991/
- ^
Senolytic drugs: from discovery to translation https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7405395/
- ^
The serial cultivation of human diploid strains https://pubmed.ncbi.nlm.nih.gov/13905658/
- ^
Senescence-Associated Secretory Phenotypes Reveal Cell-Nonautonomous Functions of Oncogenic RAS and the p53 Tumor Suppressor https://journals.plos.org/plosbiology/article?id=10.1371/journal.pbio.0060301
- ^
Treatment with the BCL-2/BCL-xL inhibitor senolytic drug ABT263/Navitoclax improves functional hyperemia in aged mice https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8599595/
- ^
Whole-body senescent cell clearance alleviates age-related brain inflammation and cognitive impairment in mice https://pubmed.ncbi.nlm.nih.gov/33470505
- ^
Obesity-Induced Cellular Senescence Drives Anxiety and Impairs Neurogenesis https://pubmed.ncbi.nlm.nih.gov/30612898/
- ^
Senolytic treatment rescues blunted muscle hypertrophy in old mice https://link.springer.com/article/10.1007/s11357-022-00542-2
- ^
Senolytics Improve Physical Function and Increase Lifespan in Old Age https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6082705/
- ^
Senolytics in idiopathic pulmonary fibrosis: Results from a first-in-human, open-label, pilot study https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6412088/
- ^
Senolytics decrease senescent cells in humans: Preliminary report from a clinical trial of Dasatinib plus Quercetin in individuals with diabetic kidney disease https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6796530/
- ^
Age-Related Macular Degeneration: A Scientometric Analysis https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4458325/
- ^
Age-Related Macular Degeneration https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9369215/
- ^
Intravitreal anti-VEGF agents and cardiovascular risk https://pubmed.ncbi.nlm.nih.gov/31848994/
- ^
lifespan.io Rejuvenation Roadmap https://www.lifespan.io/road-maps/the-rejuvenation-roadmap/
- ^
Kelsey Moody | Macular Degeneration https://www.youtube.com/watch?v=CIIvKhJO-m8
- ^
Thymic involution and rising disease incidence with age https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5828591/
- ^
Dr. Greg Fahy – Rejuvenating the Thymus to Prevent Age-related Diseases https://www.lifespan.io/news/rejuvenating-the-thymus/
- ^
Reversal of epigenetic aging and immunosenescent trends in humans https://onlinelibrary.wiley.com/doi/full/10.1111/acel.13028
- ^
Greg Fahy, Intervene Immune | Thymus Rejuvenation Progress Update https://www.youtube.com/watch?v=KukRAXnNOJM (edited transcript: https://foresight.org/summary/greg-fahy-intervene-immune-thymus-rejuvenation-progress-update/)
- ^
- ^
7-Ketocholesterol in disease and aging https://www.sciencedirect.com/science/article/pii/S2213231719311759?via%3Dihub
- ^
Cyclodextrin dimers: A versatile approach to optimizing encapsulation and their application to therapeutic extraction of toxic oxysterols https://pubmed.ncbi.nlm.nih.gov/33839224/
- ^
Cyclodextrin dimers for the remediation of atherosclerotic plaque https://www.atherosclerosis-journal.com/article/S0021-9150(22)00798-5/fulltext
- ^
Erosion of the Epigenetic Landscape and Loss of Cellular Identity as a Cause of Aging in Mammals https://www.biorxiv.org/content/10.1101/808642v1
- ^
Toward a unified theory of aging and regeneration https://www.researchgate.net/publication/335454143_Toward_a_unified_theory_of_aging_and_regeneration
- ^
Reprogramming to recover youthful epigenetic information and restore vision https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7752134/
- ^
Premature termination of reprogramming in vivo leads to cancer development through altered epigenetic regulation https://pubmed.ncbi.nlm.nih.gov/24529372/
- ^
Partial reprogramming deep dive: the good, bad, and partially unresolved https://www.adanguyenx.com/blog/partial-reprogramming
- ^
- ^
The Hallmarks of Aging https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3836174/
- ^
Extending human healthspan and longevity: a symposium report https://pubmed.ncbi.nlm.nih.gov/34498278/
- ^
The Fountain of Youth? The Quest for Aging Therapies (Subcommittee on Investigations and Oversight) https://youtu.be/Sm5K7WqgsDQ?t=355
- ^
Fountain of Youth Hearing Charter https://science.house.gov/imo/media/doc/9.15.2022%20Fountain%20of%20Youth%20Hearing%20Charter.pdf
- ^
James Kirkland on growing interest from political figures https://www.youtube.com/watch?v=VxAZw1Xoa3g&t=2296s
- ^
Tackling ageing may be best way to prevent multiple chronic conditions from developing in older people https://theconversation.com/tackling-ageing-may-be-best-way-to-prevent-multiple-chronic-conditions-from-developing-in-older-people-174645
- ^
Jim Mellon: Longevity could be the best investment you ever make https://longevity.technology/news/jim-mellon-longevity-could-be-the-best-investment-you-ever-make/
- ^
Treatment with the BCL-2/BCL-xL inhibitor senolytic drug ABT263/Navitoclax improves functional hyperemia in aged mice https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8599595/
The point is not tractability or preference for either outcome, but timelines. It’s possible to solve ageing “manually”. But it’s looking like AGI will very likely get here first, as a matter of forecasting, not because it’s a good or safe thing for this to happen, and not because it needs to happen in order to invent anti-ageing. Nanotech is in the same place as anti-ageing, it’s also possible to figure out “manually”, but it’s also going to take more time than AGI, and therefore it’s AGI that gets to figure it out.
Point taken. I guess the main difference for me is that with age reversal, we’ve got a framework that makes sense and de-mystifies it, and it implies that if we just do this and this and this and this then the problem should be solved. We can actually see a path between where we are right now and where we want to be. Do we have something like that with AGI, or is it more a matter of “these language models are starting to look pretty smart”? I’m not saying I would bet against AGI, the way things are going… but I wouldn’t want to rely on it without a rational model of it, either.
For what it’s worth, as someone with incredibly short time expectation until we get the big one over in AI land, I don’t think “ask agi to figure it out” is going to be how it feels to solve aging using agi. I expect it to look more like supercharging exactly this research plan you outline with extremely advanced bio simulation. And I expect that AI safety will look like biosecurity, in large part because I don’t think it could possibly look another way—as ai advances it is looking more and more like a field of silicon biology.
Try this post. Basically, everything is too easy recently, with many roads leading to progress. And very recently, there are plausible roadmaps that don’t require any new discoveries (which would otherwise take unknown amount of time), just some engineering. It’s no longer insane (though not yet likely, I’d give it 8%) for AGI to be done in two years even without secret projects or unexpected technical breakthroughs. (By AGI I mean a point where AI becomes able to teach itself any skills that don’t fall out of its low level learning algorithm on their own, but it hasn’t yet learned much in this way.)
Alignment looks relatively hopeless, but at the same time if AGI is something along the lines of ChatGPT, it’s more likely to be somewhat human-like and possibly won’t cause outright extinction, even if it takes away most of the resources in future lightcone that humanity could’ve gotten for itself if it was magically much better at coordination and took its time to figure out alignment or uploading.
UK-based researchers interested in this subject, and potentially international collaborators, could apply to the recently-announced UKRI funding opportunity:
https://www.ukri.org/opportunity/ageing-research-development-awards/
On values: while I share your desire that we could live arbitrary old, we should also take care of the unintended consequences. The one that always come to mind is: how will we spare space for the youths? I do think satisfying solutions exists (for example, elders past 150 could be require to take increasingly long vampire-style naps), but I encourage you to think and write your own solution on how to make ultra-high longevity sustainable at the societal level, as it’ll almost always be the core objection of your most motivated opponents.
On hard reality is a bitch: the biologist in me is very confident that it’s terribly misleading to think biological ageing as a simple accumulation of damages. I suspect you’re making a categorical mistake by confusing what you wish to achieve (that one day we will consider ageing as unimportant as scratching a knee cap) with how simple animal physiology accept to be.
A few paradigmatic counter-points:
Cancer is not just damaged cells: they are subjected to natural selection, which makes fighting cancer look more like trench warefare than changing broken tiles.
In a close vein, we should expect some virus (some of which might be dormant in our own genome, or within the genome of our own microbiote) or bacteria to have learned when the host is old enough it’s time to strike for your own fitness purposes (I suspect that’s the main reason why transfusing young blood benefits older organisms -by fooling the wannabe scavengers into believing you would fight back as hard as if you’d risk missing your most productive breeding years)
CRPS is proof that a minor tissue damage can lead to a disease that is not only far worse, but also persisting long after the initial damage is fully repaired. In the same vein, most chronic back pain persist without any persisting evidence for tissue damage, and you might want to count PTSD as well.
Progeria and menopause strongly suggest that aging is, at least partially, under genetic control.
I’m unusually chill when it comes to population, both over and under. I’m not enormously concerned by how many people there are, I’m more concerned by how healthy the existing people are, and how healthy the environment is, both of which are mostly orthogonal to population and depend primarily on technological development. It’s important to note that fertility rates are generally declining worldwide, seemingly in tandem with economic development. The most economically developed countries generally have below-replacement fertility rates, and are facing depopulation plus highly inverted population pyramids (high ratio of sick, dependent, aged people) if something doesn’t change. In places where fertility is below two children per woman, you could abolish death completely and population will plateau, since each generation produces fewer children than the one before, so you get a geometric series with r < 1. Thus, the only study I’m aware of that analyses the demographic consequences of rejuvenation therapies predicts only slow and limited population growth (at least in Sweden).
Of course, it all depends how fertility changes. Ending reproductive senescence could allow people to postpone childbirth even further than they already do, lowering fertility rates further, or it could lead to people having more children throughout their greatly extended lifetimes. I suspect the former will occur, but time will tell.
Oh, I hope I didn’t give the impression that this was simple. One of my core points is that ageing cannot be reduced to any single target for intervention, there is no way around the fact that ageing is many-faceted and will require complex combination therapies to address. I only assert that there will be some combination of damage which, if eliminated, will elicit healthy life extension, and that we have some well educated guesses as to what those are and how to go about fixing them, and that doing so can only be good for people even if damage identified by SENS platform is not in fact comprehensive.
Counter-counter-points:
Yes, cancer is hard and I glossed over it. Partly it will be mitigated by immune system rejuvenation, since immune surveillance plays a huge role in cancer suppression. Dealing with mitochondrial dysfunction should also reduce cancer incidence, by lowing the amount of free-radical assault on DNA. Aside from that though, there are exciting things happening in actual cancer therapy: cancer immunotherapy (works very well in blood cancers, might scale to solid cancers), THIO by MAIA Biotechnology (rapidly kills cells that express high levels of telomerase, which most cancers do by necessity), Lou Hawthorne’s NaNots (can safely remove stuff from the blood, can be used to soak up the soluble immune system inhibitors that tumours have to use to protect themselves from the immune system, and finally, Michael Levin’s lab have managed to suppress cancers using ion channel drugs, along with opening a whole new perspective on what cancer fundamentally is.
The effects rejuvenating effects of parabiosis are due to either good things in the young blood, or dilution / removal of bad things (e.g. inflammatory signalling molecules) in the old blood. The debate continues, but I believe consensus is leaning towards the latter, since you can achieve similar results just by diluting the blood with saline-albumin [1,2].
Function follows form. If there are diseases that aren’t associated with any obvious damage, then that only means we’ve yet to identify what the damage is. Machines do what they do because their structure; if they malfunction, then there must some change somewhere in the structure that causes it, and whatever that change is, we call it damage. Remember that damage is defined very broadly, it doesn’t have to be what you’d think of as “wear-and-tear” necessarily—it could be something like over-sensitisation of a particular type of neuron in the case of CRPS, for example.
Progeria (assuming you mean Hutchinson-Gilford syndrome) is a mutation in a critical nuclear envelope protein which causes rapid and widespread damage of many forms, since it’s such a critical component that’s defective. It’s thought of as “premature ageing” since its symptoms resemble accelerated normal ageing, probably because “widespread damage of many forms” is what normal ageing is, but that doesn’t mean that the damage involved in progeria is the same as in normal ageing (though there’s probably some overlap). As for menopause, it’s kind of a moot point to me whether a change is “under genetic control” (difficult to define since everything is ultimately determined by genes anyway) or not. Thymic involution appears to be a programmed developmental change, but we still call it damage, because it causes a loss of function (inability to make new naive T-cells). We don’t much care how damage happens, only how to reverse it.
Why would fertility per woman stay the same when childbearing lifespan is increased? It seems more likely to me that fertility per woman per year would stay the same—have a kid or two, then a few decades doing other things, then another kid or two and so on. And this leads to exponential growth (as long as fertility/woman/year > 0).
Is that really conter counter? Levin’s idea on long range communication fits well with the ideas of cancer as learning system, even better than natural selection alone. Also, the impact of diluting blood seems 100% compatible with the idea that it’s diluting an ageing marker (indeed inflammatory molecules are excellent candidates).
These definitions are imho too forgiving.: if we define damage as loss of health, then sure « removing damage » will tautologically cause good health. If we define damage as material defects, which I think is closer to your original intent, then maladaptative memories (of the affective system in PTSD, of the pain system in CRPS, of the immune system….) can cause a loss of function without a lasting role for material damages (beside killing oneself when it’s no longer possible to cope with this level of pain|suffering)
“Material”? I don’t think it’s useful to distinguish between material and immaterial change, the point is that the change is maladaptive. If your hard drive gets corrupted preventing your computer from booting then we still call that damage, even though it seems less material than, say, shooting the PSU. And ultimately, data and code are material anyway, whether they’re represented by patterns of magnetic polarisation or changes to neuronal sensitivity or connectivity or whatever.
Very good points. The obvious solutions are either really low birth rates and/or aggressive expansion into space. Both of which are hard.
In a certain sense it’s correct to say that resetting the whole body to a 25 year olds level would fix most health problems. The problem with this is that it’s also the solution to fixing a broken vase. Biology has a very nasty habit of turning out to be even more complicated than you expected when you start digging deeper. Cleaning up doesn’t have to suffice—there are various intra- and extracellular (i.e. hormones) interactions, cascades and what not which would also have to be set appropriately.
The biologist in me would also like to point out the existence of zombie genes, which start expressing themselves after death—more as a curiosity than a specific point—animal physiology is fascinating.
Suppose a future technological trick allows our civilisation to magically size and control anything material within a spheric bubble growing at light speed: that means what we own would grow as a polynomial (2 or 3, depending on your TOE). But polynomial growth is not enough to cope with any fixed grow rate of the population (that’s exponential), so that’s why I think amortals should play on time to make space. In permutation city, Greg Egan imagine the uploaded could play with their refreshing speed. In the context of biological immortality, taking long naps could serve the same purpose.
Always glad to see Greg Egan referenced. The important thing to me is that although population growth could be exponential (for the reasons cousin_it gave), it’s going to be very slow relative to the rate of technological progress. Unless fertility rises significantly, it’s likely to be hundreds of years before population would grow by 10x, by which point we’re well into Greg Egan territory and all bets are off anyway. So population could be a concern, but we’ll have plenty of time to address it via methods that don’t involve literally everyone dying.
On second thought, strong upvote for this answer because I think it’s key to pinpoint our divergence.
You think that we will likely be well into Greg Egan territory in a few hundred years, whereas new tools in biology are so fantastic we are a few decades to, yes immortality, but I guess you see that as a direct consequence of reaching biological universality (when we can basically at will make cells do whatever one cell can do).
To me (and, in a sense, echoing Vladimir_Nesov´s comment above) that’s the contrary: not only I expect new biological limitations to show up nearly as fast as we solve old problems (like decoding the human genome was fantastic, and fruitful, but not as fruitful as I was naively thinking at the time), but I also fully expect we will taste Greg Egan territory several decades before we will fully master our own biology.
Late late late disclaimer: I’m toying with the idea of starting a series of post called Road to amortality, so you should expect me to be biased and stubbornly attached to my ideas. 😉
To fight the latter, here’s one result that would move me toward your position: if we can print or grow any complex organ within the next decade. Do you accept this criteria as fair and to the point? Would you mind thinking of some results that would make you strongly update toward my position?
Naps would handle the amount of people walking around, but would probably require some novel approaches to ownership to work properly. Or synchronization of when people wake up? With the current norms, you’d end up with empty cities, because a large fraction of the inhabitants would be asleep at each given moment. Though magically sizing stuff would also handle that issue.
After reflexion I still don’t get your point, e.g. what problems intermittent naps would make us need new approach to ownership. Say we the people agree for sustainability purpose to set a fix number A as the number of people allowed & required to be awake, and P is the total number of people, sleeping or awake. Then everyone would have a right to be awake A/P of the years, or A/P decades within each millennia, and from that we might want to trade synchronisation with Star War MCXIV release for synchronisation with Harry upcoming new biography, the way Smith intended capitalism. What am I missing?
Assume you have a population of 1000 billion people on earth (what with the hibernation tech), with most of them sleeping at any given time, so that you only have 10 billion awake. If everyone has their own apartment/house then at any given time, only 1% of the houses will be in use. This in itself is fine, as people can simply synchronize when they wake up to have empty/full neighborhoods. But it would also require either having 100x more infrastructure to handle the larger cities (or paving over the world, or more exotic solutions), giving everyone a lot less living room (e.g. pod skyscrapers) or having shared accommodations (like hotels or shared bedrooms).
My main point is that the current approach, where a house with a large garden is the default to strive for, would be totally untenable. Which in turn would require a lot of cultural changes (people tend to like having lots of room for themselves). This by no means invalidates the idea of napping, it’s just something that would have to be handled.
I’m guessing compounded interest could also be troublesome in the long run, e.g. you start a savings account now, and someone else starts in a million years—that would introduce some scary inequality. For the same reason that the older the vampire, the more powerful.
Ok, thanks for clarifying (I misunderstood « approaches » as implying new economical system). Yes, that scenario would need us to change some of our habits, for example we could share home with P/A family member, or rent it while sleeping.
Interesting thought. On the other hand, the more sleepers, the more capital, the lower the interest rate. And what kind of bank could we trust for one million years?
You may well turn out to be correct—biology is indeed fiendishly complex and still very poorly understood, and it may turn out that clearing the damage types identified by the SENS platform is insufficient for comprehensive rejuvenation. However, I’ve tried to separate that particular claim from a different, more defensible, more immediately relevant one: that damage repair should become our main approach to medical research in a world where infectious disease is largely conquered, and most suffering is due to (mostly age related) chronic illnesses. Most bodily disorders these days are caused not by infection by an external pathogen, but by damage to the body itself, most of which is self-inflected by ordinary metabolic processes. Yet for some reason, we continue to treat the (often arbitrarily defined) diseases themselves, as though they were infectious diseases, instead of even trying to repair the damage that causes them. This must change, and it is changing. To me, damage repair is a first and foremost a new, fundamentally different approach to medicine, one that emphasizes fixing things that are obviously broken, which I expect to work much better than the old paradigm of treating diseases separately. The whole “ageing” thing is almost secondary to me. We’ve literally not been fixing people’s bodies this entire time, and now people are finally trying to fix a bunch of obviously broken things, that’s why I’m excited.
I like the parts of the post I’ve read so far, and I’m just making a local argument to this specific bit.
People have been fixing people’s bodies insofar as they can, since the dawn of medicine. They’ve been setting bones, stitching wounds, treating or preventing inflammation and autoimmune reactions, and more recently, destroying or removing cancer and transplanting organs.
What unites SENS interventions is that they require sophisticated cellular and subcellular therapies that depend on the stack of biomedical technologies we’ve produced at an accelerating pace over the last century. Cellular senescence was discovered in vitro a little over 60 years ago, and as recently as 1996, a Berkeley cancer biologist was still writing in Cell that “a limited number of in vivo experiments… strongly suggest that cellular senescence is not an artifact of culture,” i.e. that it takes place in the body, not just in a dish, though the potential mechanistic links between senescence as a tumor suppression mechanism and driver of aging were already well-known. We only sequenced the human genome in 2003, and Crispr-CAS9 has only been around since 2012.
Point being that we’ve been trying to fix people’s bodies for millennia, but we’ve only had the scientific knowledge and bioengineering technology that might potentially allow us to treat the cellular and subcellular precursors of homeostatic breakdown (“aging”) for a matter of years.
Yes we’ve always been trying to fix damage—anything that restores function must fix damage somehow—but it’s a matter of what we consider to be damage, i.e. “bad stuff that we should try to fix because it would restore function”. Historically we’ve focused on trauma, infection and cancer, and although we’ve known about age-related changes like lipofuscin accumulation for a long time, it’s only recently that we started thinking of them as potential targets. Gerontology has historically been a field of basic science, with few gerontologists willing to venture that we could even in principle do something about age-related changes until very recently. They were too afraid to challenge the deeply held notion that ageing is normal, natural and fundamentally immutable. I’m not without sympathy though—anyone who had made that claim would have been attacked and likely would have lost their livelihood—Aubrey de Grey was only able to do it because he was financially independent.
If you look at things like atherosclerosis and AMD, both of which have long been known to be driven by the accumulation of toxic metabolites, I think we could and should have started working on the root causes of these diseases much earlier than we did. Sure, we’re only now figuring out how to remove 7KC and A2E, but that’s because we only just started working on it! Likewise, we’ve known about thymic involution for a long time and it’s always been clear that it damages your immune system in the long run, so why is it that only Greg Fahy is working on fixing it, and why does he get so little funding that his trials have to be funded by their own participants? We declared war on cancer long ago, when our models and tools were still hopelessly crude, and because of that we are further advanced now than we would have been otherwise.
Point taken that this is all extremely difficult and ambitious, and it’s not entirely unreasonable that researchers have been intimidated by that. Rejuvenation is indeed highly dependent on very recent technological breakthroughs, and those new capabilities are a huge part of why this shift is occurring. In my defense, there is a bit where I say
Perhaps I could have stressed that more. To whatever extent there is blame, I place it more on grant committees than on medical researchers. The stuff SENS works on is all high-risk high-reward, which public purse-holders and investors are both cagey about—that’s why it all has to be philanthropically funded. For example, the idea to copy mitochondrial DNA into the nucleus where it is safer (which I ignored completely in the post) has been around for a long time, but SENS had to work on it because no one else would.
Anyway, I don’t want to fixate on whose fault things were. The point is that for whatever reason, we were pursuing a broken paradigm of “one disease one target one drug”, which was never going to work because the diseases were not naturally separable things and their root causes mostly lay in fundamental age-related changes, which we are now beginning to target, and it seems likely to work.
Agreed, I like this elaboration. As I see it, the argument really is that we’ve been neglecting preventative medicine in favor of treating disease after it has become symptomatic. This is a familiar critique that normal doctors and laypeople already subscribe to, and showing that anti-aging medicine is really just another familiar form of preventative medicine (which we have historically neglected) will make more immediate sense than claiming that “we haven’t been fixing people’s bodies” which is only true in the specific sense you just articulated.
Along with that is emphasizing that it’s normal and natural to use preventative medicine. You brush your teeth, you try to eat a good diet and get enough sleep and exercise, you might stake preventative statins or blood thinners or get LASEK. If you’ll do all these things to maintain your health, then why not take low-dose rapamycin? It’s really going to be about normalizing the use of pill-form preventatives at an earlier age, and breaking the association between pills and “being sick.” Instead, it’s about creating an association between pills and “maintaining health.”
It’s both prevention and cure—prevent disease by reversing damage before it gets bad enough to cause problems, but if you already have a chronic disease, then reversing the damage that causes it will be the only way to cure it (though prevention is better of course).
I agree the preventative medicine angle is a good one that people will buy easily, but you can make the same argument against it—that we’ve always been trying to prevent disease just as we’ve always been trying to fix damage.
It’s important to note that statins, blood thinners and rapamycin are not damage repair—they’re not useless, but I think damage repair will make them obsolete. These approaches focus on slowing the buildup of damage rather than reversing damage that’s already there. The problem is that a) this tries to modify human metabolism to “run more cleanly”, which is super difficult and prone to unforeseen consequences and b) you have to take these medicines every day, which makes it all the more dangerous. Statins are well known to have side effects, and rapamycin is an immunosuppressant, which unsurprisingly has a lot of side effects too. You don’t want to take this stuff every day.
The reason people associate things like statins with “being sick” is that they don’t actually make you less sick, they just slow the progression of a disease while causing side effects. Damage repair is far less prone to side effects because it targets stuff that’s definitely not supposed to be there instead of trying to change the way the body works. You won’t get side effects from removing atheromatous plaques (so long as that’s all the treatment does do), but you do get side effects from mucking around with liver chemistry. And because ageing damage accumulates so slowly, you’ll only have to take these therapies every 10 years or so (eventually, once they’re mature). And of course, because it reverses damage instead of merely slowing it, you’ll actually feel, look and be healthier and fitter after the treatment. That’s why I say it’s a new kind of medicine—the public are absolutely not used to medicine that makes them feel younger after they take it.
That’s a reasonable point of view. I don’t think we should be certain that the effects of rapamycin at high doses will be reflective of its effects at low doses, which is why we need to test it. This era is all about precision medicine, figuring out how to control dosing, release, and specific delivery in the context of much better knowledge of how these drugs affect the body to cut side effects and enhance benefit.
The heuristic of leaning toward occasional damage repair by engineered interventions rather than continuous damage slowdowns by manipulating evolved biochemistry makes sense, but so does the heuristic of focusing on an available tool that we have extensive data works pre-clinically right now. I think the “don’t mess with evolution” heuristic is oversubscribed for antagonistic pleiotropy and declining selection pressure with age reasons when it comes to anti-aging medicine.
All the same, I expect that over time we’ll come up with a wide range of both preventative and damage reversal interventions, perhaps along SENS lines. But in that context, a damage-slowing drug (perhaps rapamycin) that might reduce the frequency of the need for damage reversal therapies will be highly valuable, and particularly because it may well be the cheapest and most accessible option to get started, especially in countries that don’t yet have fully developed medical systems..
Totally agree and am glad you wrote this post
This is very interesting. “We should increase healthspans” is a much more palatable sentiment than “Let’s reach longevity escape velocity”. If it turns out healthspan aligns well with longevity, we don’t need to flip everyone’s mindsets about the potential for life extension; we can start by simply pointing to interventions that aim to mitigate the multi-morbidity of elderly people.
“Healthy ageing” doesn’t disambiguate between chronological age and metabolic health the way you try to do in this post, but it can still serve as a sentiment that’s easy to fit inside the Overton window.
100% agree the messaging should focus on health rather than lifespan—not only because it’s far less controversial (most people want to be healthy), but because it’s true: we work directly on health, of which longevity is but a side effect. Glad you picked up on the multi-morbidity part too, tackling age-related sickness as a whole by focusing on fundamental ageing damage rather than treating diseases separately is crucial. Probably we’ll be talking about morbidity compression for a while yet; this is a crux that allows us to discuss medicine that actually works without having to acknowledge the Biblical-scale consequences of it. At some point though, laboratory results will become so compelling that the delusion collapses, and then all hell will break loose.
It can’t not. People don’t die because they get old, they die because they get sick.
It appears not, we have the studies that show training can reverse those epigenetic clocks, via stress adaptation, and the studies that show exercise accelerates the rate of actual cellular aging. As you would put it, exercise trades fitness for what you are calling health. I know that wasn’t your intention to have the field taken over by fitness buffs, but the flawed nature of the clocks appear to have enabled this. I don’t think the name is a problem, the problem is what you measured. I don’t consider a 60 y/o face, with 40 y/o muscles, after 50 birthdays health worth billions in investment. Slaves who worked fields were fit as fiddles, they were strong until they collapsed abruptly at the end of middle age. The case for the most minimal fitness intervention you can get away with appears to be aligned with maximum healthspan and lifepsan but not fitness.
While the term “healthspan” can be useful for public messaging it is not necessary to use it instead of “lifespan” as study after study shows. When the word “lifespan” is used in the correct context people are very willing to embrace even radical lifespan extension. It seems prudent to combine both concepts.
Asked “If doctors developed a pill that enabled you to live forever at your current age, would you take it?” a surprising number of people turned out to be hardcore life extensionists: “There were no differences by age...Among young adults, 40.0% indicated they would not take the pill, 34.2% indicated they would take the pill, and 25.8% indicated they were unsure.”
Barnett, Michael D., and Jessica H. Helphrey. “Who wants to live forever? Age cohort differences in attitudes toward life extension.” Journal of Aging Studies 57 (2021): 100931.
When do the cells with sufficiently long telomeres run out? Removing senescent cells sounds good, but if all the cells have a built-in recursion limit, at some point there won’t be any cells with sufficiently long telomeres left in the body. Assuming a non-decreasing division rate, this puts a time limit on longevity after this intervention.
(is this time limit just really large compared to current lifespans, so we can just figure it out later?)
EDIT: nevermind, the answer to this seems to be in the “Epigenetic reprogramming” section; TLDR pluripotent stem cells
Not all cells in the adult body do divide, most of them I think divide only rarely if ever. Cells that divide more regularly generally express telomerase to keep their telomeres from running out. Telomeres running out may still be an issue though, so there are people looking at ways of lengthening them via telomerase expression.
Hi Phil,
Loved you essay, so interesting, exciting, fun & educative, thank you for it :)
Here is a few points I would like to make as they come “as is” in my limited brain:
1) I totally subscribe to it as well as to the many “longevicists” (or whatever it is called, is there a name for it?) before you like Aubrey about addressing human aging as a disease/condition/self-damage/… that has to be addressed directly. As would determined any simple “root cause analysis” why indeed not spending much more resources into directly addressing the root cause rather than all its individual numerous symptoms (i.e. all the diseases/damage which result from the aging process)?
2) The obvious dangers of experimenting with aging therapy could be solved using simulation, there is already some work on going trying to digitally simulate at molecular level some organs like liver, brain, etc… once we have a fully functioning human simulation at atom/molecular levels, it will be much safer to unleash/test any kind of aging therapy on it. But then some people will argue that if we have a working atom-by-atom biological simulation of the human body (including its brain) then we have reached the TS and we can simply accelerate that simulation as much as we can to make that human body and brain simulation work on solving its own aging process :) I love these conundrums about human body/brain simulations :)
3) This leads me to the 2 separate approaches of solving aging that have been mentioned here:
3a) Trying to solve aging using the technology we currently have.
3b) Just work on SI (Super intelligence) and wait until we have SI to then ask SI to solve human aging.
I would say wait not combining 3a) and 3b) together into
3c) Using “centaur intelligence” (as in Kasparov “centaur chess”) to try to solve human aging by using the combined force of human research and AI/AGI together to work on solving human aging as it would have the following benefits:
• Working efficiently & effectively on human aging right now.
• Applying AI/AGI to a hard problem like human aging would also likely lead to further advances in AI/AGI research.
(bullet point character shortcut tip: on Windows: [Alt]-[Numpad 7] for those who do not yet know!)
4) If we have SI and we ask it to solve human aging I guess one possible and quite rational answer that it would give is: “OMG the human body is so lame, why not digitalize/store/upload the human brain/mind/consciousness (and the old human body if you really feel like it) data in the cloud and then embody that brain/mind/consciousness into whatever much better body/bodies than a lame natural human body full of design flaws and limitations? And if you really want me to solve that lame natural human body aging, yes of course I can do that, here are 1000 different solutions from “least invasive/transformative” to “most invasive/transformative” to implement (...)” :)
5) Just one small detail I have spotted, at some point you mention than Covid-19 IFR is 2%, may I ask you where you get that number from? From what I’ve read through the pandemic this number started at around 1% (specially it is the IFR not the CFR) and has decreased ever since with probably an average of 0.5% through the pandemic so far. But if I am wrong please let me know where you got your 2% number from so you make me less wrong :)
Indeed—people are finally thinking “what if ageing has something to do with all the age-related disease?” This is great, so long as you remember that “ageing” is not just one single root cause of age-related disease; rather, it’s a multitude of self-inflicted injuries the body slowly accumulates, which combine to make us frail and disease-prone.
Simulations of that fidelity level would indeed be ridiculously powerful tools, but I don’t know how long it’ll take to reach that level. Also, with a true full-body molecular simulation you’d have the ethical problem that a simulation at that level of detail is for all intents and purposes a human being, and may no longer be ethical to experiment on. The strength of damage repair as a medicinal paradigm is that it exposes a whole host of targets that we can safely go after, confident that doing so will improve function without having a full understanding of how the body works. Often we try to treat disease by changing the way the body works (e.g. statins), but this is very hard to do without side-effects because of how complex and inter-connected the body’s systems are. But the things I call “damage” are age-related changes that are unambiguously bad for you and can in principle be reversed. Doing so might not cure all age-related diseases, but it should prevent them all, since by definition they tend not to occur in people who don’t have a lifetime of age-related changes.
People are absolutely applying the centaur-intelligence thing to ageing already (e.g. Gero, Altos, In Silico), indeed I think all current applications of AI are working in synergy with human intelligence, and I hope it stays that way for as long as possible. It’s good that we are indeed able to benefit from (what currently passes for) AI long before it reaches the level where we can just ask ChatGPT “how do I cure ageing” and it just tells us.
What matters here is what we want. For now, I quite enjoy being made out of meat, and I think most other people do too. Our desires are what they are, and they don’t require justifying, to AGI or to anyone else. Of course, such transformative alterations/extensions to our selves will no doubt be unlocked one day, and I could happily live in a world where people modify themselves in all sorts of different ways, one step at a time, on their own terms, as and when they feel like it.
It’s almost certainly me that’s wrong here—there have been lots of different IFRs quoted so I picked 2% as the highest I could remember hearing, just to be conservative. Lower IFR would strengthen the argument I was making there, and indeed the true number is almost certainly much lower due to e.g. asymptomatic infections.
More a question than comment or critique. (and still reading through but will probably be over multiple reads)
The Senolytics section comes across a bit like all senescent cells are bad so if we could just kill them all we’d be doing a good thing. But my understanding is that they also play a role in healthy body functions. Is that also your understanding here?
Largely related to the above, the framing of the post seems that of body as a machine but I’m wondering if that is the best framing. Perhaps body as a ecosystem might be better. I don’t think it changes any of the main points you make (that I’ve read) but perhaps suggests following the machine metaphor might be limiting, and in some cases point in the wrong direction. Does that seem right to you?
And thanks for posting and the summarization of current state as you see it.
From what I’ve read, the healthy roles they play are a) during early/embryonic development and b) in wound healing. So, don’t give senolytics to embryos or people healing from wounds I guess. Also, there’s a paper (summary here) showing that it’s possible to regain the wound-healing benefit of SCs in mice that are engineered not to create SCs, just by manually applying a single growth factor that SCs secrete into wounds. So it seems unlikely that the beneficial roles of SCs are a show-stopper, particularly because those beneficial effects are more associated with short-lived SCs rather than the ones that linger and accumulate.
I find it fascinating to think of the body as an ecosystem (e.g. cells competing for resources, occupying niches), but I use the machine analogy because it emphasizes that there’s an overall structure and function that can be degraded. What does it mean for an ecosystem to age or decline, how do you define the health of an ecosystem?
You can imagine an ecosystem <---> machine axis, where it’s more like an ecosystem when you have independent entities competing for their own survival, and more like a machine when they work more closely together to act as one. In this sense, I think metazoans are both ecosystem and machine. But much if not most of the damage that drives ageing is at the level of individual cells rather than whole organism, and it makes more sense to think of individual cells as machines.
One way in which the ecosystem view is helpful is that it emphasizes that dead or damaged cells (e.g. senescent cells) can be destroyed and replaced by the division of healthy cells. That’s something you couldn’t do in a non-ecosystem-like-machine, such as a car, and it’s a major benefit—replacement of old cells by new is really the best form of damage repair since you “repair” all the damage at once that way.
Ray Peat claims the Hayflick limit is nonsense, but… It’s Ray Peat, so apply salt. http://raypeat.com/articles/articles/stemcells.shtml
There are papers showing senescent cells in humans with signs of shortened telomeres and replicative stress (e.g. [1,2]), so I wouldn’t say the Hayflick limit is nonsense or irrelevant in humans. But there is perhaps a broader point that the Hayflick limit / telomere erosion has been over-hyped as the fundamental driver of ageing. Case in point, I once talked to a guy who told me “Immortality is impossible, because: telomeres”.
The problem is that telomere erosion tells a simple and compelling story about what ageing is, like every cell has a built-in clock that prevents us living too long. From skimming the article, the point Ray Peat seems to be making, in a rather snarky and conspiratorial way, is that it’s much more complicated than that, which is true. The point I’m making in this post is that there is no primary mechanism or process which is or causes ageing. Ageing is driven by a multitude of unavoidable cellular and molecular changes, but the list is finite, and fixing it is a tractable engineering problem.
Talking about aging without mentioning the Gompertz–Makeham law is like talking about physics without mentioning the law of conservation of energy, impossible to take seriously. Strongly downvoted for exuberant incompetence/irrationality. One example where you make factually false statements:
No, it does not. The rate of decline is exponential. The heath decline rate is an exponent of that.
I often talk about physics without talking about the law of conservation of energy. My guess is 99% of physics discussions don’t happen to mention that law, important as it is. This is meant to be an informal overview, not an introductory textbook on longevity.
Again this is clearly meant to be a non-technical overview. The intent is clearly the informal meaning of exponential, i.e. getting faster with time, not the technical meaning of c^x.
I could be wrong, but it seems to me you’ve reacted negatively to this post for some reason, and are justifying it with what are clearly not particularly strong reasons. I think it’s worth analysing why that is.