It feels so long ago that Covid and health were my beat, and what everyone often thought about all day, rather than AI. Yet the beat goes on. With Scott Alexander at long last giving us what I expect to be effectively the semi-final words on the Rootclaim debate, it seemed time to do this again.
Bad News
I know no methodical way to find a good, let alone great, therapist.
Cate Hall: One reason it’s so hard to find a good therapist is that all the elite ones market themselves as coaches.
As a commentor points out, therapists who can’t make it also market as coaches or similar, so even if Cate’s claim is true then it is tough.
My actual impression is that the elite therapists largely do not market themselves at all. They instead work on referrals and reputation. So you have to know someone who knows. They used to market, then they filled up and did not have to, so they stopped. Even if they do some marketing, seeing the marketing copy won’t easily differentiate them from other therapists. There are many reasons why our usual internet approach of reviews is mostly useless here. Even with AI, I am guessing we currently lack enough data to give you good recommendations from feedback alone.
I wish this man the best of luck. I hope he finds the answers and does not die, and that this helps the rest of us also not die.
Alas, I am not expecting much. His concept of ‘rate of aging’ does not strike me as how any of this is likely to work, nor does addressing joint health seem likely to much extend life or generalize. His techniques do not target any of the terminal aging issues. A lot of it seems clearly aimed at being healthy now, feeling and looking younger now. Which is great, but I do not expect it to buy much in the longer term.
Also one must note that the accusations in the responses to the above-linked thread about his personal actions are not great. But I would not let that sully his efforts to not die or help others not die.
I can’t help but notice the parallel to AI safety. I see Johnson as doing lots of mundane health work, to make himself healthier now. Which is great, although if that’s all it is then the full routine is obviously a bit much. Most people should do more of such things. The problem is that Johnson is expecting this to translate into defeating aging, which I very much do not expect.
Gene therapy cures first case of congenital deafness. Woo-hoo! Imagine what else we could do with gene therapies if we were ‘ethically’ allowed to do so. It is a sign of the times that I expected much reaction to this to be hostile both on the ‘how dare you mess with genetics’ front and also the ‘how dare you make someone not deaf’ front.
The Battle of the Bulge
A ‘vaccine-like’ version of Wegovy is on the drawing board at Novo Nordisk (Stat+). If you are convinced you need this permanently it would be a lot cheaper and easier in this form, but this is the kind of thing you want to be able to reverse, especially as technology improves. Consider as parallel, an IUD is great technology but would be much worse if you could not later remove it.
Page Six: Tracy Morgan says he ‘gained 40 pounds’ on weight-loss drugs: I can ‘out-eat Ozempic’
“It cuts my appetite in half,” the 55-year-old told Hoda Kotb and Jenna Bush Hager on the “Today” show in August 2023.
We used to eat a lot more, including more starch and sugar, without becoming obese, including people who did limited physical activity. According to these statistics, quite a lot more. Yes, we eat some new unhealthy things, but when people cut those things out without cutting calories, they do not typically lose dramatic amounts of weight.
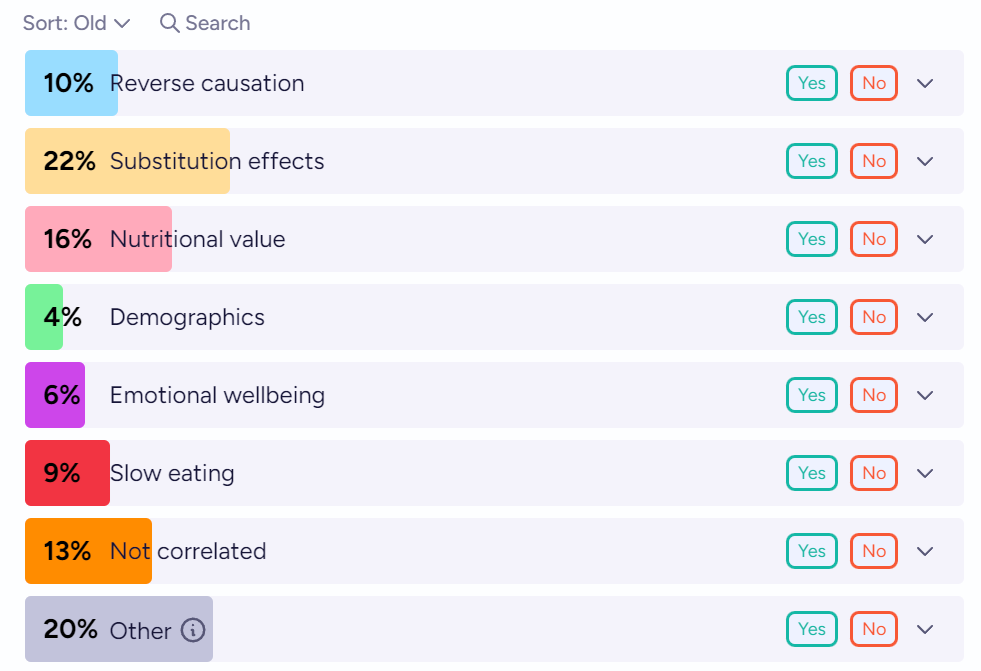
All right, why do the studies find ice cream is good for you, again? As a reminder the Atlantic dug into this a year ago, and now Manifold gives us some options, will resolve by subjective weighing of factors.
My money continues to be on substitution effects, with a side of several of the other things. Ice cream lets you buy joy, and buy having had dessert, at very little cost in calories, nutrition or health. No, it’s not great for you, but it’s not in the same category as other desserts like cake or cookies, and it substitutes for them while reducing caloric intake.
I am not about to short a 13% for five years, but I very much expect this result to continue to replicate. And I do think that this is one of the easier ways to improve your diet, to substitute ice cream for other desserts.
Andrea Peterson (WSJ): Scientists agree broadly on what constitutes a healthy diet—heavy on veggies, fruit, whole grains and lean protein—but more research is showing that different people respond differently to the same foods, such as bread or bananas.
I would instead claim we have broad agreement as to what things we socially label as ‘healthy’ versus ‘unhealthy,’ with little if any actual understanding of what is actually healthy or unhealthy, and the broad expectation among the wise that the answers vary greatly between individuals.
Elizabeth and his fellow participants spend two weeks each on three different diets. One is high fat and low carb; another is low on added sugars and heavy on vegetables, along with fruit, fish, poultry, eggs and dairy; a third ishigh in ultra-processed foods and added sugars.
This at best lets us compare those three options to each other under highly unnatural conditions, where the scientists apply great pressure to ensure everyone eats exactly the right things, and that have to severely alter people’s physical activity levels. A lot of why some diets succeed and others fail is how people actually act in practice, including impact on exercise. Knowing what set of foods in exactly what quantities and consumption patterns would be good if someone theoretically ate exactly that way is nice, but of not so much practical value.
Also, they are going to put each person on each diet for only two weeks? What is even the point? Yes, they draw blood a lot, measure heart rates, take other measures. Those are highly noisy metrics at best, that tell us little about long term impacts.
This does not seem like $189 million well spent. I cannot imagine a result that would cause me to change my consumption or much update my beliefs, in any direction.
Keto Carnivore: [losing weight] not hard compared to being fat, in pain, chronically fatigued, or anxious/depressed/psychotic. Those things are extremely motivating. It’s only hard if it doesn’t work, or the body is fighting it (like caloric restriction without satiation, or constant cravings).
confirm. Do you know how much willpower I need to do a pretty strict ketogenic diet?
0. Because the alternative is not having a career/life and feeling like shit all the time from sleep deprivation.
When it obviously works, motivation is not an issue.
To clarify, I have a very rare and specific circadian rhythm disorder that therapeutic keto fixes. 99.99% of people don’t have this issue and therefore won’t get the same benefits I do.
Motivation is not an issue for me, in the sense that I have no doubt that I will continue to do what it takes to keep the weight off.
That does not mean it is easy. It is not easy. It is hard. Not every day. Not every hour. But often, yes, it is hard, the road is long. But yeah, the alternative is so obviously worse that I know I will do whatever it takes, if it looks like I might slip.
Support Anti-Aging Research
‘‘What we wish we knew entering the aging field.’ I hear optimistic things that we will start to see the first real progress soon, but it is not clear people wouldn’t say those things anyway. It certainly seems plausible we could start making rapid progress soon. Aging is a disease. Cure it.
Variably Effective Altruism
Ken Griffin donates $400 million to cancer hospital Sloan Kettering. Not the most effective altruism available, but still, what a mensch.
Periodic Reminders (You Should Know This Already)
Sulfur dioxide in particular is a huge deal. The estimate here is that a 1 ppb drop in levels, a 10% decline in pollution, would increase life expectancy by a whopping 1.2 years. Huge if even partially true, I have not looked into the science.
HIPPA in practice is a really dumb law, a relic of a time when digital communications did not exist. The benefits of being able to email and text doctors vastly exceed the costs, and obviously so. Other places like the UK don’t have it and it’s much better.
The story of PEPFAR, and how it turned out to be dramatically effective to do HIV treatment instead of HIV prevention, against the advice of economists. Back then there were no EAs, but the economists were making remarkably EA-like arguments, while making classic errors like citing studies showing very low cost estimates per life saved for prevention that failed to replicate, including ignoring existing failed replications. And they failed to understand that the moral case for treatment allowed expansion of the budget and also that treatment halted transmission, and thus was also prevention.
In many senses, it is clear that Bush ‘got lucky’ here, with the transmission effect and adherence rates exceeding any reasonable expectations, while prevention via traditional methods seems to have proven even less effective than we might have expected. If I had to take away three key lessons, they would be that you need to do larger scale empiricism to see what works and not count on small studies, and that you should care a lot about making the moral or obvious case for what you are doing, because budgets for good causes are never fixed. People adjust them based on how excited they are to participate. And I do not think this is stupid behavior on anyone’s part, focusing on things where you score clear visible wins guards against a lot of failure modes, even at potential large efficiency costs, while usually still being more than efficient enough to be worth doing on its own merits.
Henry: TIL there was a company that sold a baby sock with an spo2 monitor that sent a push notification if your baby stopped breathing until the FDA forced them to stop selling them because only doctors should be able to see a blood oxygen number.
> The FDA objection was based on the fact that the wearable had the capacity to relay a live display of a baby’s heart rate and oxygen levels, which is critical data that a doctor should interpret, especially in vulnerable populations.
FDA delenda est.
If I try, yes, I can tell a story where people think ‘oh I do not have to check on my baby anymore because if something goes wrong the sock will tell me’ and this ends up being a bad thing. You can also tell that story about almost anything else.
Other Enemies of Life
Some very silly people argue that it is not preventing schizophrenia unless you do so in a particular individual, if you do it via polygenic selection then it is ‘replacement.’ Scott Alexander does his standard way overthinking it via excruciating detail method of showing why this is rather dumb.
90% of junior doctors in South Korea strike to protest against doctors. Specially, against admitting 2,000 more students each year to medical schools. One can say ‘in-group loyalty’ or ‘enlightened self-interest’ if one wants. Or realize this is straight up mafia or cartel behavior, and make it 5,000.
Brian Patrick Moore: Good thing we don’t have some crazy thing like this in the US
Of all the low hanging fruits in health care, ‘lots of capable people want to be doctors and we should train more of them to be doctors’ has to be the lowest hanging of all.
Covid Postmortems
Vaccine mandates for health care workers worsened worker shortages on net, the ‘I don’t want to get vaccinated or told what to do’ effect was bigger than the ‘I am safer now’ effect, claiming a 6% decline in healthcare employment. Marginal Revolution summarized this as the mandate backfiring. We do see that a cost was paid here. It is not obvious the cost is not worthwhile, and also if someone in healthcare would quit rather than be vaccinated one questions whether you wanted them working that job.
From Paxlovid to vaccines to masks to ventilation. Public health sounded (and still sounds like) a used car salesman for many different reasons:
Data seems crafted to feed the pitch rather than the pitch crafted by data. Overly optimistic claims weren’t well-supported by data, risks of Covid were communicated uniformly which meant the risks to young people were exaggerated, and potential vaccine harms were dismissed. Later, when it was time to pitch boosters, public health pivoted on a dime to tell us vaccine protection wanes quickly. How did we get here?
Data mistakes …
Messaging inaccuracies. …
Mixing advocacy with scientific communication … The latest example was a long Covid discussion at a recent congressional hearing, and one of the top long Covid doctors saying, “The burden of disease from long Covid is on par with the burden of cancer and heart disease.”
I would give people more credit. Focusing on what things ‘sound like’ was a lot of what got us into this mess.
The issue wasn’t that everything ‘sounded’ like a sales pitch.
The problem was that everything was a sales pitch.
People are not scientific experts, but they can recognize a sales pitch.
The polite way to describe what happened was ’scientists and doctors from Fauci on down decided to primarily operate as Simulacra Level 2 operators who said what they thought would cause the behaviors they wanted. They did not care whether their statements matched the truth of the physical world, except insofar as this would cause people to react badly.
As for this last item, I mean, there is a lot of selection bias in who becomes a ‘top long Covid doctor’ so it is no surprise that he was up there testifying (in a mask in 2024) that long Covid is on par with the burden of cancer and heart disease, a comment that makes absolutely zero sense.
Indeed, statements like that are not ‘mixing advocacy with scientific communication.’ My term for them is Obvious Nonsense, and the impolite word would be ‘lying.’
Information that would have been helpful was never provided
Indeed, ‘ethicists’ and other experts worked hard to ensure that we never found out much key information, and that we failed to communicate other highly useful informat we did know or damn well have enough to take a guess about, in ways that ordinary people found infuriating and could not help but notice was intentional.
This has been going on forever in medicine, better to tell you nothing than information ‘experts’ worry you won’t interpret or react to ‘properly,’ and better not to gather information if there is a local ethical concern no matter the cost of ignorance, such as months (or in other cases years) without a vaccine.
A disconnect between what I experienced on the ground and the narrative I was hearing
As in, Covid-19 in most cases wasn’t that scary in practice, and people noticed. I do think this one was difficult to handle. You have something that is 95%-99% to be essentially fine (depending on your threshold for fine) but will sometimes kill you. People’s heuristics are not equipped to handle it.
She concludes that some things are improving. But it is too little, too late. Damage is mostly done, and no one is paying attention anymore, and also they are still pushing more boosters. But this is at least the start of a real reckoning.
As an example of this all continuing: I have been told that The New York Times fact checks its editorials, and when I wrote an editorial I felt fact checked, but clearly it does not insist on those checks in any meaningful sense, since they published an op-ed claiming the Covid vaccine saved 3 million lives in America in its first two years. That makes zero sense. America has only 331.9 million people, and the IFR for Covid-19 on first infection is well under 1% even for the unvaccinated. The vaccines were amazing and saved a lot of lives. Making grandiose false claims does not help convince people of that.
He is still presenting More Lockdowns as something that would have been wise?
If the Australian right could implement hard lockdowns to control the virus, I believe the American right could have as well. This probably would have saved a ton of lives. Australia and other countries with tougher lockdown policies saw dramatically lower mortality.
Or maybe not?
Even a really successful lockdown regime couldn’t be sustained forever, and there was a price to pay in Australia and Finland and everywhere else once you opened up.
I mean, yes those other countries had lower mortality, but did America have the prerequisites to make such policies sustainable, where they work well enough you can loosen them and they still work and so on? I think very clearly no. Trying to lock down harder here would have been a deeply bad idea, because for better and also for worse we lacked the state and civilizational capacity to pull it off.
Then we have these two points, which seem directly contradictory? I think the second one is right and the first is wrong. The hypocrisy was a really huge deal.
I think the specific hypocrisy of some progressive public health figures endorsing the Floyd protests is somewhat overblown.
…
After Floyd, it became completely inconceivable that any liberal jurisdiction in America would actually enforce any kind of tough Covid rules.
He makes this good note.
Speaking of drift, I think an under-discussed aspect of the Biden administration is they initiated a bunch of rules right when they took office and vaccine distribution was just starting and had no plan to phase them out, seemingly ever. When they got sued over the airplane mask mandate, they fought in court to maintain it.
At minimum this was a missed opportunity to show reasonableness and competence. At worst, this was a true-colors moment for many people, who remember even if they don’t realize they remember.
Matt also points out that there has been no reckoning for our failures. America utterly failed to make tests available in reasonable fashion. Everyone agrees on this, and no one is trying to address the reasons that happened. The whole series of disingenuous mask policies and communications also has had no reckoning. And while Democrats had an advantage on Covid in 2020, their later policies did not make sense, pissed people off and destroyed that advantage.
(I mean, I could of course be hired to do so, but I advise you strongly not to do that.)
To illustrate how bad an idea that would be, Scott Alexander offers us the highlights from the comments and deals with various additional arguments. It ends with, essentially, Rootclaim saying that Scott Alexander did not invest enough time in the process and does not know how to do probability theory, and oh this would all be sorted out otherwise. Whether or not they are right, that is about as big a ‘there be dragons and also tsuris’ sign as I’ve ever seen.
The one note I will make, but hold weakly, is that it seems like people could do a much better job of accounting for correlated errors, model uncertainty or meta uncertainty in their probability calculations.
As in, rather than pick one odds ratio for the location of the outbreak being at the wet market, one should have a distribution over possible correct odds ratios, and then see how much those correlate with correct odds ratios in other places. Not only am I not sure what to make of this one rather central piece of offered evidence, who is right about the right way to treat that claim would move me a lot on who is right about the right way to treat a lot of other claims, as well. The practical takeaway is that, without any desire to wade into the question of who is right about any particular details or overall, it seems like everyone (even when not trolling) is acting too confident based on what they think about the component arguments, including Scott’s 90% zoonosis.
My actual core thinking is still that either zoonosis or a lab leak could counterfactually have quite easily caused a pandemic that looks like Covid-19, our current ongoing practices at labs like Wuhan put as at substantial risk for lab leaks that cause pandemics that could easily be far worse than Covid-19.
I do not see any good arguments that a lab leak or zoonosis couldn’t both cause similar pandemics, everyone is merely arguing over which caused the Covid-19 pandemic in particular. And I claim that this fact is much more important than whether Covid-19 in particular was a lab leak.
Rupa Subramanya (The Free Press): Zoraya ter Beek, 28, expects to be euthanized in early May.
Her plan, she said, is to be cremated.
“I did not want to burden my partner with having to keep the grave tidy,” ter Beek texted me. “We have not picked an urn yet, but that will be my new house!”
She added an urn emoji after “house!”
Ter Beek, who lives in a little Dutch town near the German border, once had ambitions to become a psychiatrist, but she was never able to muster the will to finish school or start a career. She said she was hobbled by her depression and autism and borderline personality disorder. Now she was tired of living—despite, she said, being in love with her boyfriend, a 40-year-old IT programmer, and living in a nice house with their two cats.
She recalled her psychiatrist telling her that they had tried everything, that “there’s nothing more we can do for you. It’s never gonna get any better.”
At that point, she said, she decided to die. “I was always very clear that if it doesn’t get better, I can’t do this anymore.”
…
“I’m seeing euthanasia as some sort of acceptable option brought to the table by physicians, by psychiatrists, when previously it was the ultimate last resort,” Stef Groenewoud, a healthcare ethicist at Theological University Kampen, in the Netherlands, told me. “I see the phenomenon especially in people with psychiatric diseases, and especially young people with psychiatric disorders, where the healthcare professional seems to give up on them more easily than before.”
Theo Boer, a healthcare ethics professor at Protestant Theological University in Groningen, served for a decade on a euthanasia review board in the Netherlands. “I entered the review committee in 2005, and I was there until 2014,” Boer told me. “In those years, I saw the Dutch euthanasia practice evolve from death being a last resort to death being a default option.” He ultimately resigned.
Once again, we seem unable to be able to reach a compromise between ‘this is not allowed’ and ‘this is fully fine and often actively encouraged.’
This is especially true when anything in-between would be locally short-term worse for those directly involved, no matter what the longer-term or broader implications.
We have now run the experiment on euthanasia far enough to observe (still preliminary, but also reasonably conclusive) results on what happens when you fully accept option two. I am ready to go ahead and say that, if we have to choose one extreme or the other, I choose ‘this is not allowed.’
Ideally I would not go with the extreme. I would instead choose a relatively light ‘this is not allowed’ where in practice we mostly look the other way. But assisting you would still be taking on real legal risk if others decided you did something wrong, and that risk would increase if you were sufficiently brazen that your actions weakened the norms against suicide or you were seen as in any way applying pressure.
However, I worry that if the norms are insufficiently strong, they fail to be an equilibrium, and we end up with de facto suicide booths and medical professionals suggesting euthanasia to free up their budgets and relatives trying to get you out of the way or who want their inheritance early, a lot of ‘oh then kill yourself’ as if that is a reasonable thing to do, and life being cheap.
Saloni: Fascinating read about the world’s newest most expensive drug ($4M)
A one-off treatment for metachromatic leukodystrophy, a rare genetic condition where kids develop motor & neurological disease, and most die in childhood.
42% of untreated died before 6 yo versus 0% of treated.
Kelsey Piper: $4M is of course an eye-popping amount of money, but this is apparently 1⁄40,000 US births. Would you pay $100 to guarantee that, if your baby is one of them, they will likely be healthy and live a normal life instead of dying a slow horrible death over several years? I would!
So it’s worth it at $4M, and also the price will come down, and also lots of other people will benefit from the medical developments that come with it. What a win.
Dave Karsten: This just feels straightforward reasonable give usual costing for regulatory interventions if it’s a “saves 0.58 human lifetimes per dose” price (Yes obvi other hazards await any patient in the future and maybe you should NPV the value also, but you get my point).
The disease is progressive. The 58% of children who live to age 6 are not going to get anything like full quality of life, with declining function over time.
So yes, assuming this is a full cure then this does seem worth it for America, on the principle that a life saved is worth about $10 million. In theory we should be willing to pay at least $5 million for this drug, possibly up to $10 million, before it would cost more than it is worth.
Thus, one could say this is priced roughly correctly. Why shouldn’t a monopolist be charing roughly half of consumer surplus, especially if we want to incentivize creating more such products? Seems like about the right reward.
(Obviously, one could say EA-style things about how that money might be better spent. I am confident telling those people they are thinking on the wrong margin.)
A psychiatrist overstepping their qualifications by saying “It’s never gonna get any better” ((particularly when the source of the suffering is at least partly BPD, for which it’s commonly known that symptoms can get better in someone’s 40s)) clearly should never happen.
However, I’d imagine that most mental health professionals would be extremely careful when making statements about whether there’s hope for things to get better. In fact, there are probably guidelines around that.
Maybe it didn’t happen this way at all: I notice I’m confused.
This could just be careless reporting by the newspaper.
The article says:
She recalled her psychiatrist telling her that they had tried everything, that “there’s nothing more we can do for you. It’s never gonna get any better.”
Was it really the psychiatrist who added “It’s never gonna get any better,” or was it just that the psychiatrist said “There’s nothing more we can do for you,” and then Zoraya herself (the person seeking assisted suicide) told the reporters her conclusion “It’s never going to get any better,” and the reporters wrote it as though she ascribed those words to the psychiatrist?
In any case, this isn’t a proper “watch” (“assisted suicide watch”) if you only report when you find articles that make the whole thing seem slippery-slopy. (And there’s also a question of “how much is it actually like that?” vs “How much is it in the reporting” – maybe the reporter had their own biases in writing it like that. For all we know, this person, Zoraya, has had this plan for ever since she was a teenager, and gave herself 25 years to stop feeling suicidal, and now it’s been enough. And the reporter just chose to highlight a few things that sound dramatic, like the bit about not wanting to inconvenience the boyfriend with having to keep the grave tidy.)
I feel like the response here should be: Think hard about what sorts of guidelines we can create for doctors or mental health professionals to protect against risks of sliding down a slippery slope. It’s worth taking some risks because it seems really bad as well to err in the other direction (as many countries and cultures still do). Besides, it’s not straightforwardly evidence of a slippery slope simply because the numbers went up or seem “startling,” as the article claims. These developments can just as plausibly be viewed as evidence for, “startlingly many people suffer unnecessarily and unacceptably without these laws.” You have to look into the details to figure out which one it is, and it’s gonna be partly a values question rather than something we can settle empirically.
There are other written-about cases like Lauren Hoeve quite recently, also from Netherlands, who’d suffered from debilitating severe myalgic encephalomyelitis (ME) for five years and began her assisted suicide application in 2022. Anyone interested in this topic should probably go through more of these accounts and read sources directly from the people themselves (like blogposts explaining their decision) rather than just media reporting about it.
Theo Boer, a healthcare ethics professor at Protestant Theological University in Groningen, served for a decade on a euthanasia review board in the Netherlands. “I entered the review committee in 2005, and I was there until 2014,” Boer told me. “In those years, I saw the Dutch euthanasia practice evolve from death being a last resort to death being a default option.” He ultimately resigned.
I found a submission by this Theo Boer for the UK parliament, where he explains his reasons for now opposing euthanasia in more detail.
He writes:
It is well known that British advocates of assisted dying argue for a more restricted law than is found in the low countries. Here is my prediction: any law that allows assisted dying will come to be experienced as an injustice and will be challenged in the courts. Why only euthanasia for terminally ill patients, who have access to an ever widening array of palliative care and whose suffering will be relatively short, whereas chronic patients may suffer more intensely and much longer? Why exclude psychiatric patients, many of whom are suffering most heartbreakingly of all? Why only an assisted death for people suffering from a disease, and not for those suffering from irremediable meaninglessness, alienation, loneliness, from life itself? We are presently seeing how in the years 2016-2023 Canada’s Medical Assistance in Dying (MAiD), from being euthanasia for terminal patients only, has evolved into an assisted death for patients whose chronic disease has become unbearable due to shortage of healthcare(Douthat 2022).
This is a “slope” of sorts, but I think it’s not a bad one. The arguments for extending the practice all seem reasonable. What matters is, “are people suffering?” and, “are they right that there’s not enough hope for them to justify continued suffering?”
Regarding pressure/being pressured, I thought this part was interesting:
This brings me to the second question: how to protect vulnerable citizens? Different from what is presently going on in Canada, I do not yet see a specific risk for citizens who by many are considered vulnerable – homeless, underinsured, people on welfare, people with disabilities. Although these groups are present in those who get euthanasia in the Netherlands, it is not my impression that they are overrepresented. If any group is well represented in the euthanasia numbers, it is the better-off, the healthy-aging population, the higher educated. In our research on practice variation, we found that in regions where the average experienced health is higher, the euthanasia numbers are also higher. In places where people on average are better off, obviously serious threats to their wellbeing tend to be more often a reason for a euthanasia request than in places where people are more used to dealing with life’s different hardships. This leads me to adopt a different definition of vulnerability, a vulnerability that may be found in all social and economic groups, from top to bottom: one of despair, meaninglessness, social isolation, feeling redundant. It may apply to wealthy citizens in a villa with woodblock floors and a grand piano, whose children have their businesses elsewhere and whose friends are either dead or institutionalized, just as much as to a single disabled woman on welfare. Anyone under this shadow of despair may make a euthanasia request, and there is no way a government can prevent this kind of vulnerability to motivate a euthanasia request, since the autonomous citizens are not under any other pressure than their own, that is, their own incapacity to face life’s harder episodes. “Life has always been a feast for me,” an elderly man whose euthanasia I assessed, “and that’s how it should end for me.”
I’d be curious to figure out why it is exactly that requests for euthanasia are higher in demographs where people tend to be better off/suffering less.
That said, I’m not at all convinced that this would prove that there’s something horribly wrong going on with these developments after legalization of assisted suicide. (Still, I’d be curious to investigate this further.)
Reading this account, it feels to me like Theo Boer has a problem with death intrinsically, as opposed to only having a problem with death when a person has for-themselves good/strong reasons to continue to want to live. That’s not an outlook I agree with.
“Their own incapacity to face life’s harder episodes” is a question-begging phrasing. For all we know, many people who choose assisted suicide would voluntarily chose to continue with their suffering if there was more at stake that they cared about! For instance, if they learned that by continuing to suffer, they’d solve world poverty, they might continue to suffer. It seems wrong, then, to say they’re “incapable,” when the real reason is more about how they don’t want it enough. It’s their life, so their decision.
“Since the autonomous citizens are not under any other pressure than their own” – this is also an interesting perspective. He seems to be conceding that no matter how much society and relatives try to reassure chronically ill or disabled elderly people that they’re still valued and cared about (something we absolutely must emphasize or work towards if it isn’t everywhere the case!), those people will struggle with worries of being a burden. That’s unfortunate, but also very natural. It’s how I would feel too. But people who feel that way don’t necessarily jump right towards considering assisted suicide! Consider two different cases:
You still enjoy life/are happy.
You have been feeling suicidal for many years, and there’s no realistic hope for things to get better.
In which of these cases is “worries about being a burden” (even if you know on some level that these worries probably don’t accurately reflect the reality of the views of your caretakers or loved ones) a bigger reason to sway your decision towards wanting euthanasia? Obviously, it is in the second case, where you lack positive reasons to stay alive, so negative reasons weigh more comparatively, even if they’re quite weak in absolute terms. In fact, what if “what will other people think” had been the primary motivation that kept you wanting to live for a long time, as long as you could provide more value for your relatives or loved ones? Is there not also something disconcerting about that? (To underscore this point, many people who are depressed write that the main reason they don’t consider suicide more seriously is because of what it would do to their relatives and loved ones. If you want to see for yourself, you can read reddit threads on this for examples of people’s suicidal ideation.)
“Life has always been a feast for me,” an elderly man whose euthanasia I assessed, “and that’s how it should end for me.”
This quote comes at the end of a passage that was all about “pressure,” but it has nothing to do with pressure anymore, nor does it have to do with being “incapable of facing life’s hardship.” Instead, it just sounds like this person disagrees about the view that “facing life’s hardship” for no upside is something that’s a virtue or otherwise important/right to do. This is more like an expression of a philosophy that life can be completed (see also the ending of the series ‘The Good Place,’) or, somewhat differently, that there’s no need to prolong it after the best (and still-good) times are now over. If that’s someone’s attitude, let them have it.
Overall, I respect Theo Boer for both the work he’s done for terminally ill patients in the early stages of the assisted suicide program in the Netherlands and for speaking out against the assisted suicide practice after it went in a direction that he no longer could support. At the same time, I think he has an attitude towards the topic that I don’t agree with. In my view, he doesn’t seem to take seriously how bad it is to suffer, and especially, how bad and pointlesss it is to suffer for no good reason.
It might well be true that doctors and mental health professionals are now okay with assisted suicide as a solution too quickly (without trying other avenues first), but I’m not sure I’d trust Theo Boer’s judgment on this, given the significant differences in our points of view. In any case, I acknowledge this is a risk and that we should take steps to make sure this doesn’t occur or doesn’t become too strong of an issue (and people who decide to go through with it should be well-informed about other options and encouraged to try these other options in case they haven’t already been doing this to no success for many years).
This doesn’t engage with the significant downsides of such a policy that Zvi mentions.
There are definite questions about the cost/benefits to allowing euthanasia, even though we wish to allow it, especially when we as a society are young in our ability to handle it.
Glossing the only significant feature being ‘torturing people’ ignores:
the very significant costs of people dying, which is compounded by the question of what equilibrium the mental/social availability of euthanasia is like
the typical LessWrong beliefs about how good technology will get in the coming years/decades. Once we have a better understanding of humans, massively improving whatever is causing them to suffer whether through medical, social, or other means, becomes more and more actionable
what the actual distribution of suffering is, I expect most are not at the level we/I would call torture even though it is very unpleasant (there’s a meaningful difference between suicidally depressed and someone who has a disease that causes them pain every waking moment, and variations within those)
Being allowed to die is an important choice to let people make, but it does have to be a considered look at how much harm such an option being easily available causes. If it is disputed how likely society is to end up in a bad equilibrium like the post describes, then that’s notable, but it would be good to see argument for/against instead.
(Edit: I don’t entirely like my reply, but I think it is important to push back against trivial rounding off of important issues. Especially on LW.)
I agree my gloss on it is not a substantive engagement, but rather a reminder of what I consider a crucial consideration. Policies that elide horrific suffering are the norm. Part of the point is that suffering, being not available to external quantification, must be left up to the individual whenever possible. Many objections to utilitarianism involve its frequent attempts to obviate subjective effects when this isn’t appropriate.
Suffering is already on most reader’s minds, as it is the central advocating reason behind euthanasia — and for good reason.
I agree that policies which cause or ignore suffering, when they could very well avoid such with more work, are unfortunately common. However, those are often not utilitarian policies; and similarly many objections to various implementations of utilitarianism and even classic “do what seems the obviously right action” are that they ignore significant second-order effects. Policies that don’t quantify what unfortunate incentives they give are common, and often originators of much suffering.
What form society/culture is allowed/encouraged to take, shapes itself further for decades to come, and so can be a very significant cost to many people if we roll straight ahead like in the possible scenario you originally quoted.
Suffering is not directly available to external quantification, but that holds true for ~all pieces of what humans value/disvalue, like happiness, experiencing new things, etcetera. We can quantify these, even if it is nontrivial. None of what I said is obviating suffering, but rather comparing it to other costs and pieces of information that make euthanasia less valuable (like advancing medical technology).
Huge numbers of people are forced to resort to illegal methods of suicide creating legal, emotional, financial, and logistics problems for their loved ones, on top of the additional grief to the suicidee personally.
I suspect a large (possibly not dominant) part of the ice cream effect is required preptime triggering myopic discounting. If eating ice cream at home, you need to take it out of the freezer at least a few minutes before eating it; this means that if your comfort food of choice is ice cream, you’ll only eat it if it seems like a legitimately good idea (‘a moment of weakness’ becomes ‘like 10min of weakness’, a higher bar for cravings to clear).
If eating ice cream at home, you need to take it out of the freezer at least a few minutes before eating it
I’m curious whether this is true for most people. (I don’t eat ice cream any more, but back when I occasionally did, I don’t think I ever made a point of taking it out early and letting it sit. Is the point that it’s initially too hard to scoop?)
What I actually usually do is move it from the freezer to the refrigerator like 15min before I eat it, so the change in temperature is more predictable and evenly distributed (instead of some parts being melted while others stay too cold).
Is the point that it’s initially too hard to scoop?
That and it being too cold to properly enjoy the taste.
(The votes on my original comment make me think most people are less concerned about their dessert-that’s-supposed-to-be-cold being too cold. Typical-mind strikes again, I guess.)
Got it, thanks! For what it’s worth, doing it your way would probably have improved my experience, but impatience always won. (I didn’t mind the coldness, but it was a bit annoying having to effortfully hack out chunks of hard ice cream rather than smoothly scooping it, and I imagine the texture would have been nicer after a little bit of thawing. On the other hand, softer ice cream is probably easier to unwittingly overeat, if only because you can serve up larger amounts more quickly.)
I think two-axis voting is a huge improvement over one-axis voting, but in this case it’s hard to know whether people are mostly disagreeing with you on the necessary prep time, or the conclusions you drew from it.
I disagreed on prep time. Neither I nor anyone I know personally deliberately waits minutes between taking ice cream out of the freezer and serving it.
I could see hardness and lack of taste being an issue for commercial freezers that chill things to −25 C, but not a typical home kitchen freezer at more like −10 to −15 C.
Anecdata: I have in my freezer deep-frozen cake which has been there fore months. If it was in the fridge (and thus ready to eat) I would eat a piece every time I open the fridge. But I have no compulsion to further the unhealthy eating habits of future me, let that schmuck eat a proper meal instead!
Ice cream I eat directly from the freezer, so that effect is not there for me.
Hmm. My family and I always let the ice cream sit for about 10 to 15 minutes to let it soften first. Interesting to see the wide range of opinions, wasn’t even aware that wasn’t a thing.
Regarding assisted suicide, the realistic alternative in the case of the 28 year old would not be that she would live unhappily ever after. The alternative is an an unilateral suicide attempt by her.
Unilateral suicide attempts impose additional costs on society. The patient can rarely communicate their decision to anyone close to them beforehand because any confidant might have them locked up in psychiatry instead. The lack of ability to talk about any particulars with someone who knows her real identity[1], especially their therapist, will in turn mean that plenty of patients who could be dissuaded will not be dissuaded.
There is a direct cost of suicide attempts to society. Methods vary by ease of access, lethality, painfulness and impact on bystanders. Given that society defects against them by refusing to respect their choices regarding their continued existence, some patients will reciprocate and not optimize for a lack of traumatization of bystanders. Imagine being a conductor of any kind of train spotting someone lying on the tracks and knowing that you will never stop the train in time. For their loved ones, losing someone to suicide without advance warning also is a bad outcome.
I would argue that every unilateral suicide attempt normalizes further such attempts.[2] While I believe that suicide is part of a fundamental right, I also think that not pushing that idea to vulnerable populations (like lovesick teenagers) is probably a good thing. Reading that a 28yo was medically killed at the end of a long medical intervention process will probably normalize suicide in the mind of a teenager than reading that she jumped from a tall building somewhere.
Of course, medically assisted suicide for psychiatric conditions could also be a carrot to dangle in front of patients to incentivize them to participate in mental health interventions. Given that these interventions are somewhat effective, death would not have to be the default outcome. And working with patients who are there out of their free will is probably more effective than working with whatever fraction of patients survived their previous attempt and got committed for a week or a month. (Of course, I think it is important to communicate the outcome odds clearly beforehand: “after one year of interventions, two out of five patients no longer wanted to die, one only wanted to die some of the time and was denied, one dropped out of treatment and was denied and one was assisted in their suicide.” People need that info to make an informed choice!)
Realistically, I would not even bet on being able to have a frank discussion with a suicide hotline. Given that they are medical professionals, they may be required by law to try their best to prevent suicides up to and including alerting law enforcement, and phone calls are not very anonymous per default.
Assisted suicides would not necessarily legitimize unilateral suicide attempts. People can be willing to accept a thing when regulated by the state and still be against it otherwise. States collecting taxes does not legitimize protection rackets.
“The problem is that Johnson is expecting this to translate into defeating aging, which I very much do not expect.”
I’m fairly confident Johnson is betting on future tech solving aging and his goal is to live long enough to be there for it by creating measurements and therapies for the health of every organ.
From his site:
“2023: don’t die because we don’t know how long and well we can live ”
“This time, our time, right now—the early 21st century—will be defined by the radical evolution of intelligence: human, AI and biology. Our opportunity is to be this exciting future. “ https://protocol.bryanjohnson.com/
Ideally I would not go with the extreme. I would instead choose a relatively light ‘this is not allowed’ where in practice we mostly look the other way.
I’m not going to argue about assisted suicide here, but I am going to remark that cryonicists are sometimes in a dilemma where they know they have a neurodegenerative disease, which is destroying the information content of their personality, but they can’t (legally) go into cryopreservation before most of the damage has been done.

A psychiatrist overstepping their qualifications by saying “It’s never gonna get any better” ((particularly when the source of the suffering is at least partly BPD, for which it’s commonly known that symptoms can get better in someone’s 40s)) clearly should never happen.
However, I’d imagine that most mental health professionals would be extremely careful when making statements about whether there’s hope for things to get better. In fact, there are probably guidelines around that.
Maybe it didn’t happen this way at all: I notice I’m confused.
This could just be careless reporting by the newspaper.
The article says:
Was it really the psychiatrist who added “It’s never gonna get any better,” or was it just that the psychiatrist said “There’s nothing more we can do for you,” and then Zoraya herself (the person seeking assisted suicide) told the reporters her conclusion “It’s never going to get any better,” and the reporters wrote it as though she ascribed those words to the psychiatrist?
In any case, this isn’t a proper “watch” (“assisted suicide watch”) if you only report when you find articles that make the whole thing seem slippery-slopy. (And there’s also a question of “how much is it actually like that?” vs “How much is it in the reporting” – maybe the reporter had their own biases in writing it like that. For all we know, this person, Zoraya, has had this plan for ever since she was a teenager, and gave herself 25 years to stop feeling suicidal, and now it’s been enough. And the reporter just chose to highlight a few things that sound dramatic, like the bit about not wanting to inconvenience the boyfriend with having to keep the grave tidy.)
I feel like the response here should be: Think hard about what sorts of guidelines we can create for doctors or mental health professionals to protect against risks of sliding down a slippery slope. It’s worth taking some risks because it seems really bad as well to err in the other direction (as many countries and cultures still do). Besides, it’s not straightforwardly evidence of a slippery slope simply because the numbers went up or seem “startling,” as the article claims. These developments can just as plausibly be viewed as evidence for, “startlingly many people suffer unnecessarily and unacceptably without these laws.” You have to look into the details to figure out which one it is, and it’s gonna be partly a values question rather than something we can settle empirically.
There are other written-about cases like Lauren Hoeve quite recently, also from Netherlands, who’d suffered from debilitating severe myalgic encephalomyelitis (ME) for five years and began her assisted suicide application in 2022. Anyone interested in this topic should probably go through more of these accounts and read sources directly from the people themselves (like blogposts explaining their decision) rather than just media reporting about it.
You also quote this part of the article:
I found a submission by this Theo Boer for the UK parliament, where he explains his reasons for now opposing euthanasia in more detail.
He writes:
This is a “slope” of sorts, but I think it’s not a bad one. The arguments for extending the practice all seem reasonable. What matters is, “are people suffering?” and, “are they right that there’s not enough hope for them to justify continued suffering?”
Regarding pressure/being pressured, I thought this part was interesting:
I’d be curious to figure out why it is exactly that requests for euthanasia are higher in demographs where people tend to be better off/suffering less.
That said, I’m not at all convinced that this would prove that there’s something horribly wrong going on with these developments after legalization of assisted suicide. (Still, I’d be curious to investigate this further.)
Reading this account, it feels to me like Theo Boer has a problem with death intrinsically, as opposed to only having a problem with death when a person has for-themselves good/strong reasons to continue to want to live. That’s not an outlook I agree with.
“Their own incapacity to face life’s harder episodes” is a question-begging phrasing. For all we know, many people who choose assisted suicide would voluntarily chose to continue with their suffering if there was more at stake that they cared about! For instance, if they learned that by continuing to suffer, they’d solve world poverty, they might continue to suffer. It seems wrong, then, to say they’re “incapable,” when the real reason is more about how they don’t want it enough. It’s their life, so their decision.
“Since the autonomous citizens are not under any other pressure than their own” – this is also an interesting perspective. He seems to be conceding that no matter how much society and relatives try to reassure chronically ill or disabled elderly people that they’re still valued and cared about (something we absolutely must emphasize or work towards if it isn’t everywhere the case!), those people will struggle with worries of being a burden. That’s unfortunate, but also very natural. It’s how I would feel too. But people who feel that way don’t necessarily jump right towards considering assisted suicide! Consider two different cases:
You still enjoy life/are happy.
You have been feeling suicidal for many years, and there’s no realistic hope for things to get better.
In which of these cases is “worries about being a burden” (even if you know on some level that these worries probably don’t accurately reflect the reality of the views of your caretakers or loved ones) a bigger reason to sway your decision towards wanting euthanasia? Obviously, it is in the second case, where you lack positive reasons to stay alive, so negative reasons weigh more comparatively, even if they’re quite weak in absolute terms. In fact, what if “what will other people think” had been the primary motivation that kept you wanting to live for a long time, as long as you could provide more value for your relatives or loved ones? Is there not also something disconcerting about that? (To underscore this point, many people who are depressed write that the main reason they don’t consider suicide more seriously is because of what it would do to their relatives and loved ones. If you want to see for yourself, you can read reddit threads on this for examples of people’s suicidal ideation.)
This quote comes at the end of a passage that was all about “pressure,” but it has nothing to do with pressure anymore, nor does it have to do with being “incapable of facing life’s hardship.” Instead, it just sounds like this person disagrees about the view that “facing life’s hardship” for no upside is something that’s a virtue or otherwise important/right to do. This is more like an expression of a philosophy that life can be completed (see also the ending of the series ‘The Good Place,’) or, somewhat differently, that there’s no need to prolong it after the best (and still-good) times are now over. If that’s someone’s attitude, let them have it.
Overall, I respect Theo Boer for both the work he’s done for terminally ill patients in the early stages of the assisted suicide program in the Netherlands and for speaking out against the assisted suicide practice after it went in a direction that he no longer could support. At the same time, I think he has an attitude towards the topic that I don’t agree with. In my view, he doesn’t seem to take seriously how bad it is to suffer, and especially, how bad and pointlesss it is to suffer for no good reason.
It might well be true that doctors and mental health professionals are now okay with assisted suicide as a solution too quickly (without trying other avenues first), but I’m not sure I’d trust Theo Boer’s judgment on this, given the significant differences in our points of view. In any case, I acknowledge this is a risk and that we should take steps to make sure this doesn’t occur or doesn’t become too strong of an issue (and people who decide to go through with it should be well-informed about other options and encouraged to try these other options in case they haven’t already been doing this to no success for many years).
Advocating for people to be tortured is bad. We should be willing to accept quite a lot of collateral damage to avoid torturing people.
This doesn’t engage with the significant downsides of such a policy that Zvi mentions. There are definite questions about the cost/benefits to allowing euthanasia, even though we wish to allow it, especially when we as a society are young in our ability to handle it. Glossing the only significant feature being ‘torturing people’ ignores:
the very significant costs of people dying, which is compounded by the question of what equilibrium the mental/social availability of euthanasia is like
the typical LessWrong beliefs about how good technology will get in the coming years/decades. Once we have a better understanding of humans, massively improving whatever is causing them to suffer whether through medical, social, or other means, becomes more and more actionable
what the actual distribution of suffering is, I expect most are not at the level we/I would call torture even though it is very unpleasant (there’s a meaningful difference between suicidally depressed and someone who has a disease that causes them pain every waking moment, and variations within those)
Being allowed to die is an important choice to let people make, but it does have to be a considered look at how much harm such an option being easily available causes. If it is disputed how likely society is to end up in a bad equilibrium like the post describes, then that’s notable, but it would be good to see argument for/against instead.
(Edit: I don’t entirely like my reply, but I think it is important to push back against trivial rounding off of important issues. Especially on LW.)
I agree my gloss on it is not a substantive engagement, but rather a reminder of what I consider a crucial consideration. Policies that elide horrific suffering are the norm. Part of the point is that suffering, being not available to external quantification, must be left up to the individual whenever possible. Many objections to utilitarianism involve its frequent attempts to obviate subjective effects when this isn’t appropriate.
Suffering is already on most reader’s minds, as it is the central advocating reason behind euthanasia — and for good reason. I agree that policies which cause or ignore suffering, when they could very well avoid such with more work, are unfortunately common. However, those are often not utilitarian policies; and similarly many objections to various implementations of utilitarianism and even classic “do what seems the obviously right action” are that they ignore significant second-order effects. Policies that don’t quantify what unfortunate incentives they give are common, and often originators of much suffering. What form society/culture is allowed/encouraged to take, shapes itself further for decades to come, and so can be a very significant cost to many people if we roll straight ahead like in the possible scenario you originally quoted.
Suffering is not directly available to external quantification, but that holds true for ~all pieces of what humans value/disvalue, like happiness, experiencing new things, etcetera. We can quantify these, even if it is nontrivial. None of what I said is obviating suffering, but rather comparing it to other costs and pieces of information that make euthanasia less valuable (like advancing medical technology).
Huge numbers of people are forced to resort to illegal methods of suicide creating legal, emotional, financial, and logistics problems for their loved ones, on top of the additional grief to the suicidee personally.
I suspect a large (possibly not dominant) part of the ice cream effect is required preptime triggering myopic discounting. If eating ice cream at home, you need to take it out of the freezer at least a few minutes before eating it; this means that if your comfort food of choice is ice cream, you’ll only eat it if it seems like a legitimately good idea (‘a moment of weakness’ becomes ‘like 10min of weakness’, a higher bar for cravings to clear).
I’m curious whether this is true for most people. (I don’t eat ice cream any more, but back when I occasionally did, I don’t think I ever made a point of taking it out early and letting it sit. Is the point that it’s initially too hard to scoop?)
What I actually usually do is move it from the freezer to the refrigerator like 15min before I eat it, so the change in temperature is more predictable and evenly distributed (instead of some parts being melted while others stay too cold).
That and it being too cold to properly enjoy the taste.
(The votes on my original comment make me think most people are less concerned about their dessert-that’s-supposed-to-be-cold being too cold. Typical-mind strikes again, I guess.)
Got it, thanks! For what it’s worth, doing it your way would probably have improved my experience, but impatience always won. (I didn’t mind the coldness, but it was a bit annoying having to effortfully hack out chunks of hard ice cream rather than smoothly scooping it, and I imagine the texture would have been nicer after a little bit of thawing. On the other hand, softer ice cream is probably easier to unwittingly overeat, if only because you can serve up larger amounts more quickly.)
I think two-axis voting is a huge improvement over one-axis voting, but in this case it’s hard to know whether people are mostly disagreeing with you on the necessary prep time, or the conclusions you drew from it.
I disagreed on prep time. Neither I nor anyone I know personally deliberately waits minutes between taking ice cream out of the freezer and serving it.
I could see hardness and lack of taste being an issue for commercial freezers that chill things to −25 C, but not a typical home kitchen freezer at more like −10 to −15 C.
Anecdata: I have in my freezer deep-frozen cake which has been there fore months. If it was in the fridge (and thus ready to eat) I would eat a piece every time I open the fridge. But I have no compulsion to further the unhealthy eating habits of future me, let that schmuck eat a proper meal instead!
Ice cream I eat directly from the freezer, so that effect is not there for me.
Hmm. My family and I always let the ice cream sit for about 10 to 15 minutes to let it soften first. Interesting to see the wide range of opinions, wasn’t even aware that wasn’t a thing.
Regarding assisted suicide, the realistic alternative in the case of the 28 year old would not be that she would live unhappily ever after. The alternative is an an unilateral suicide attempt by her.
Unilateral suicide attempts impose additional costs on society. The patient can rarely communicate their decision to anyone close to them beforehand because any confidant might have them locked up in psychiatry instead. The lack of ability to talk about any particulars with someone who knows her real identity[1], especially their therapist, will in turn mean that plenty of patients who could be dissuaded will not be dissuaded.
There is a direct cost of suicide attempts to society. Methods vary by ease of access, lethality, painfulness and impact on bystanders. Given that society defects against them by refusing to respect their choices regarding their continued existence, some patients will reciprocate and not optimize for a lack of traumatization of bystanders. Imagine being a conductor of any kind of train spotting someone lying on the tracks and knowing that you will never stop the train in time. For their loved ones, losing someone to suicide without advance warning also is a bad outcome.
I would argue that every unilateral suicide attempt normalizes further such attempts.[2] While I believe that suicide is part of a fundamental right, I also think that not pushing that idea to vulnerable populations (like lovesick teenagers) is probably a good thing. Reading that a 28yo was medically killed at the end of a long medical intervention process will probably normalize suicide in the mind of a teenager than reading that she jumped from a tall building somewhere.
Of course, medically assisted suicide for psychiatric conditions could also be a carrot to dangle in front of patients to incentivize them to participate in mental health interventions. Given that these interventions are somewhat effective, death would not have to be the default outcome. And working with patients who are there out of their free will is probably more effective than working with whatever fraction of patients survived their previous attempt and got committed for a week or a month. (Of course, I think it is important to communicate the outcome odds clearly beforehand: “after one year of interventions, two out of five patients no longer wanted to die, one only wanted to die some of the time and was denied, one dropped out of treatment and was denied and one was assisted in their suicide.” People need that info to make an informed choice!)
Realistically, I would not even bet on being able to have a frank discussion with a suicide hotline. Given that they are medical professionals, they may be required by law to try their best to prevent suicides up to and including alerting law enforcement, and phone calls are not very anonymous per default.
Assisted suicides would not necessarily legitimize unilateral suicide attempts. People can be willing to accept a thing when regulated by the state and still be against it otherwise. States collecting taxes does not legitimize protection rackets.
That is very seldom a good idea, for reasons detailed in https://siderea.dreamwidth.org/1209794.html (if euthanasia is outlawed, only outlaws will euthanize their patients) https://www.unqualified-reservations.org/2007/04/formalist-manifesto-originally-posted/ (any circumstance where the actual norms don’t match the ostensible norms can lead to uncertainty and/or disagreements on what exactly the former are, and you don’t want that)
“The problem is that Johnson is expecting this to translate into defeating aging, which I very much do not expect.”
I’m fairly confident Johnson is betting on future tech solving aging and his goal is to live long enough to be there for it by creating measurements and therapies for the health of every organ.
From his site:
“2023: don’t die because we don’t know how long and well we can live ”
“This time, our time, right now—the early 21st century—will be defined by the radical evolution of intelligence: human, AI and biology. Our opportunity is to be this exciting future. “
https://protocol.bryanjohnson.com/
I’m not going to argue about assisted suicide here, but I am going to remark that cryonicists are sometimes in a dilemma where they know they have a neurodegenerative disease, which is destroying the information content of their personality, but they can’t (legally) go into cryopreservation before most of the damage has been done.