It’s deja vu all over again. It’s not good.
We’re focused on political fights over priority and concerns someone might jump the line, and took off for Christmas. Doctors get forty-six dollars for administering two vaccine shots, and aren’t allowed to bill for anything involved, including either office visit. The vaccine rollout is sufficiently botched that we now have to be worried about millions of doses spoiling and going unused.
It’s that bad.
Meanwhile, here we go again. The evidence from this week points to the baseline scenario laid out last week being correct. The new strain is here. It is almost certainly more infectious, probably as much more infectious as feared, and has been identified in multiple states. This is going to happen and there is nothing left capable of stopping it.
Eventually, some day, hopefully even some time in 2021, one way or another, this all will end.
Alas, it will not be tonight at midnight.
Let’s run the numbers.
The Numbers
Predictions
Last week’s prediction: 13.6% positive rate on 10.1 million tests, and an average of 2,500 deaths.
Results: 13.8% positive rate on 9.1 million tests, and an average of 2,287 deaths.
That looks like a straightforward case of not taking the drop-off from Christmas seriously enough, with deaths and tests both down 10% more than predicted, and the positive rate what you’d expect accordingly. These are temporary slash artificial drops.
But it’s hard to know when we will be back on a normal track, because things still weren’t back to normal today, and New Year’s Eve is upon us, and also the real effects of Christmas are about to arrive and the last two days positive rates are super scary.
Prediction: 14.3% positive rate on 9.7 million tests, and an average of 2,500 deaths, again with wide error bars.
Deaths
| Date | WEST | MIDWEST | SOUTH | NORTHEAST |
| Oct 29-Nov 4 | 956 | 1977 | 2309 | 613 |
| Nov 5-Nov 11 | 1089 | 2712 | 2535 | 870 |
| Nov 12-Nov 18 | 1255 | 2934 | 2818 | 1127 |
| Nov 19-Nov 25 | 1761 | 4169 | 3396 | 1714 |
| Nov 26-Dec 2 | 1628 | 3814 | 2742 | 1939 |
| Dec 3-Dec 9 | 2437 | 5508 | 4286 | 2744 |
| Dec 10-Dec 16 | 3278 | 5324 | 4376 | 3541 |
| Dec 17-Dec 23 | 3826 | 5158 | 5131 | 3772 |
| Dec 24-Dec 30 | 3363 | 3668 | 4171 | 3640 |
The Northeast generally seems to be better about reporting deaths on holidays and weekends, so the relative increase here is likely exaggerated, but also likely real. The Midwest drop likewise is too large to not be largely a function of reporting, but also too large to purely be reporting. Things peaked there some time ago.
Positive Test Percentages
| Percentages | Northeast | Midwest | South | West |
| 10⁄29 to 11⁄4 | 4.28% | 12.79% | 8.86% | 7.04% |
| 11⁄5 to 11⁄11 | 5.56% | 17.51% | 9.89% | 8.31% |
| 11⁄12 to 11⁄18 | 6.99% | 18.90% | 11.64% | 10.66% |
| 11⁄19 to 11⁄25 | 7.00% | 16.62% | 10.41% | 11.75% |
| 11⁄26 to 12⁄2 | 8.38% | 17.90% | 12.45% | 12.79% |
| 12⁄3 to 12⁄9 | 10.47% | 17.94% | 13.70% | 12.76% |
| 12⁄10 to 12⁄16 | 10.15% | 15.63% | 15.91% | 13.65% |
| 12⁄17 to 12⁄23 | 9.88% | 14.65% | 15.78% | 13.82% |
| 12⁄24 to 12⁄30 | 10.65% | 14.54% | 17.07% | 12.90% |
Like everything else, interpreting these numbers is weird, especially given this for the whole country:
| Date | %+ Today |
| 12/30/2020 | 18.7% |
| 12/29/2020 | 17.9% |
| 12/28/2020 | 12.1% |
| 12/27/2020 | 13.2% |
| 12/26/2020 | 11.0% |
| 12/25/2020 | 11.4% |
| 12/24/2020 | 13.8% |
Presumably there’s a lot of time shifting there, but there are also alternative interpretations. One of them is Christmas was really bad, and that the last two days are largely real and quite ugly. We’ll know soon enough, it felt necessary to flag it, despite the general rule that one day of data tells you nothing.
Positive Tests
| Date | WEST | MIDWEST | SOUTH | NORTHEAST |
| Nov 5-Nov 11 | 157495 | 387071 | 206380 | 108581 |
| Nov 12-Nov 18 | 211222 | 452265 | 255637 | 150724 |
| Nov 19-Nov 25 | 269230 | 435688 | 294230 | 170595 |
| Nov 26-Dec 2 | 256629 | 357102 | 294734 | 185087 |
| Dec 3-Dec 9 | 354397 | 379823 | 368596 | 263886 |
| Dec 10-Dec 16 | 415220 | 315304 | 406353 | 260863 |
| Dec 17-Dec 23 | 439493 | 271825 | 419230 | 236264 |
| Dec 24-Dec 30 | 372095 | 206671 | 373086 | 225476 |
Included for completeness more than anything else. Christmas is exactly the time not to take such numbers too seriously.
Test Counts
| Date | USA tests | Positive % | NY tests | Positive % | Cumulative Positives |
| Oct 22-Oct 28 | 6,943,470 | 7.5% | 890,185 | 1.4% | 2.67% |
| Oct 29-Nov 4 | 7,349,648 | 9.5% | 973,777 | 1.6% | 2.89% |
| Nov 5-Nov 11 | 8,285,878 | 10.7% | 1,059,559 | 2.4% | 3.16% |
| Nov 12-Nov 18 | 9,033,621 | 12.4% | 1,155,670 | 2.9% | 3.50% |
| Nov 19-Nov 25 | 10,415,393 | 11.8% | 1,373,751 | 2.9% | 3.87% |
| Nov 26-Dec 2 | 9,741,057 | 11.7% | 1,287,010 | 4.0% | 4.22% |
| Dec 3-Dec 9 | 10,458,644 | 13.9% | 1,411,142 | 4.9% | 4.66% |
| Dec 10-Dec 16 | 10,694,845 | 13.8% | 1,444,725 | 4.9% | 5.11% |
| Dec 17-Dec 23 | 10,710,356 | 13.7% | 1,440,770 | 5.1% | 5.56% |
| Dec 24-Dec 30 | 9,089,692 | 13.8% | 1,303,286 | 6.0% | 5.94% |
Covid Machine Learning Project
Up to 20.3% estimated cumulative infections by December 16, up from 19.2% as of December 9 last week, which the model still believes. Most interestingly, a report that R0 has dropped to 0.9, and things are improving for now, with infections already down almost 20% from peak.
Europe
One of these lines on that second graph is not like the others. It’s been about three weeks since the ramp-up began, so deaths should follow this coming week. If the new strain is less deadly, we’ll get the good news that way. But all of this is still distorted by Christmas, and hard to count on too much.
The English Strain: Are We F***ed? Is it Over?
Yeah, probably. Sure looks like it.
The twin central points last were that we were probably facing a much more infectious strain (70%), and that if we are fucked in this way, then it is effectively already over in the sense that our prevention efforts would be in vain.
I remain highly confident in the second claim, if the increased infectiousness is sufficiently strong. We are dealing with exponential growth, and a race condition with vaccinations and prior infections, and also looking to move into the spring and summer, so as I thought last week, I remain confident that we can probably mostly muddle through if there is small increased infectiousness (up to about 35%), at 50% I am highly skeptical we can stop this, and at 65% it’s (probably) already over.
For the first claim, my 70% probability from last week for the new strain being >50% more infectious is now 80%.
There’s also the open question of the extent to which the new strain is already circulating elsewhere. We know the strain has spread, but different orders of magnitude of existing spread are weeks different in their implications for the timeline.
The question is, how do we gather more evidence to differentiate between the various scenarios? What evidence should we look for, and how much should we update on that evidence? I started a LessWrong question thread for that, as their software is good for that use case.
Metaculus has a market up, although it asks about a relatively small threshold:
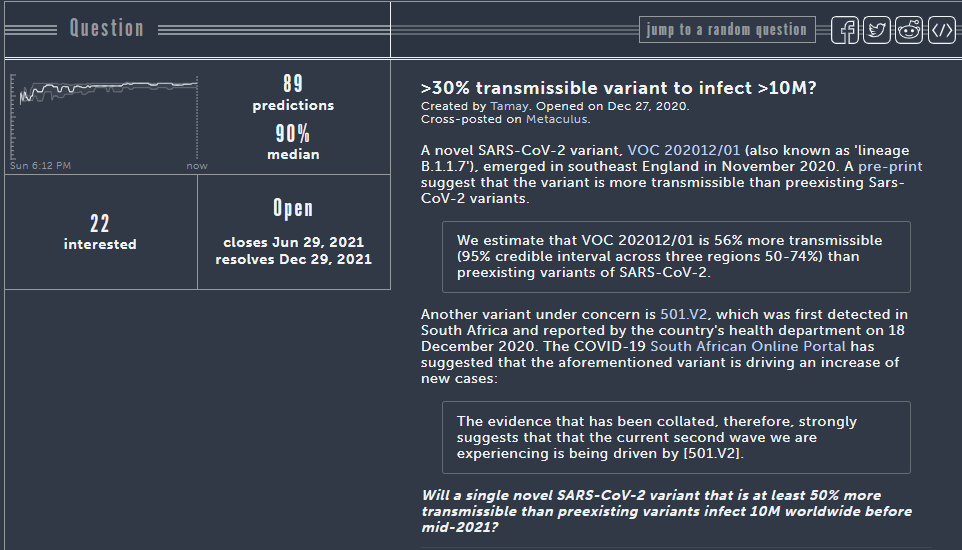
Ten million worldwide is not that much, and could easily represent a success case in the United States. This question is mostly asking “Is there a new strain that is >30% more transmissible?” Their probability of 90% reflects that, and seems fully consistent with a 70% chance of >50% more transmissible. I think we have seen enough that I strongly agree with Metaculus here that the chance of a >30% more infectious strain is very high. The more interesting question is how that translates to the chances for a >50% or >65% more infectious strain.
Metaculus also has some (entirely unsurprising) updates on spread, confirming that containment will not be a thing:
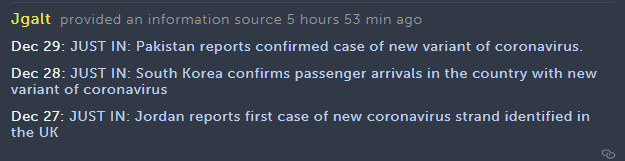

Meanwhile, in terms of how it’s going, British tourists sneak out of ski resorts to avoid retroactive quarantines.
There is still time to actually try, if one wants, though, and in some cases a non-zero chance…
Which one could contrast with this, which I do think is a slightly unfair metaphor:
Juan Cambeiro’s Twitter thread on his reasoning on this question is here, it’s long with lots of sources, pictures and reasoning, and here’s the conclusion, with numbers similar to but slightly more skeptical than my initial estimate:
Via that same page, Tom Wenseleers comes in (Twitter) with a new analysis (GitHub):
This preprint model via the LessWrong thread has a confidence interval for increased infectiousness of 50%-74%.
I found this thread informative, link to original document here:
I quote the whole thing because the end points to the newest Very Serious Person line, which is to become Very Concerned about further mutation, or even vaccine escape, and using that as a reason to limit spread. It’s the latest thing.
The reversed splits for hospitalizations and deaths in the two groups is weird, but presumably mostly random, as Kai concludes, and the big data point is that they looked at contacts for over a thousand cases, and 15.1% of contacts of the new strain became cases, versus 9.8% of contacts of the old strain became cases. That seems like a very good way to measure infectiousness. If there is a way for this to be random chance, I can’t think of a mechanism. There’s some chance those contacts became cases through other sources than the original contact, so if anything that ratio is probably an underestimate of increased infectiousness.
There’s a cool map here, but it’s hard to interact with.
This report came out on the 31st, and I haven’t had time to check if it is a duplicate or for details, but it looks like it’s giving a range of 40%-80% more infectious (Twitter source).
I checked the Good Judgment project but none of their markets seem to interact much with the question. I’ve also noticed a lot of their predictions are highly questionable. They are especially prone to wild swings of overconfidence, especially in political questions, and at least one current prediction on that page seems like it’s very, very wrong as of when I wrote this section, but I don’t want to go off topic so I won’t say more.
On December 29, the variant was found in the United States for the first time, in a Colorado man in his 20s who works at a nursing home (which is in turn a reminder that our failure to administer the vaccine quickly is going to cost many lives) and has no history of travel. So we have proof of community spread. The next day, health officials say they have found a second suspected case. It seems all but certain there are many people with the strain already in the United States. The question that will help determine our resulting timeline is, are we talking about hundreds, thousands or tens of thousands?
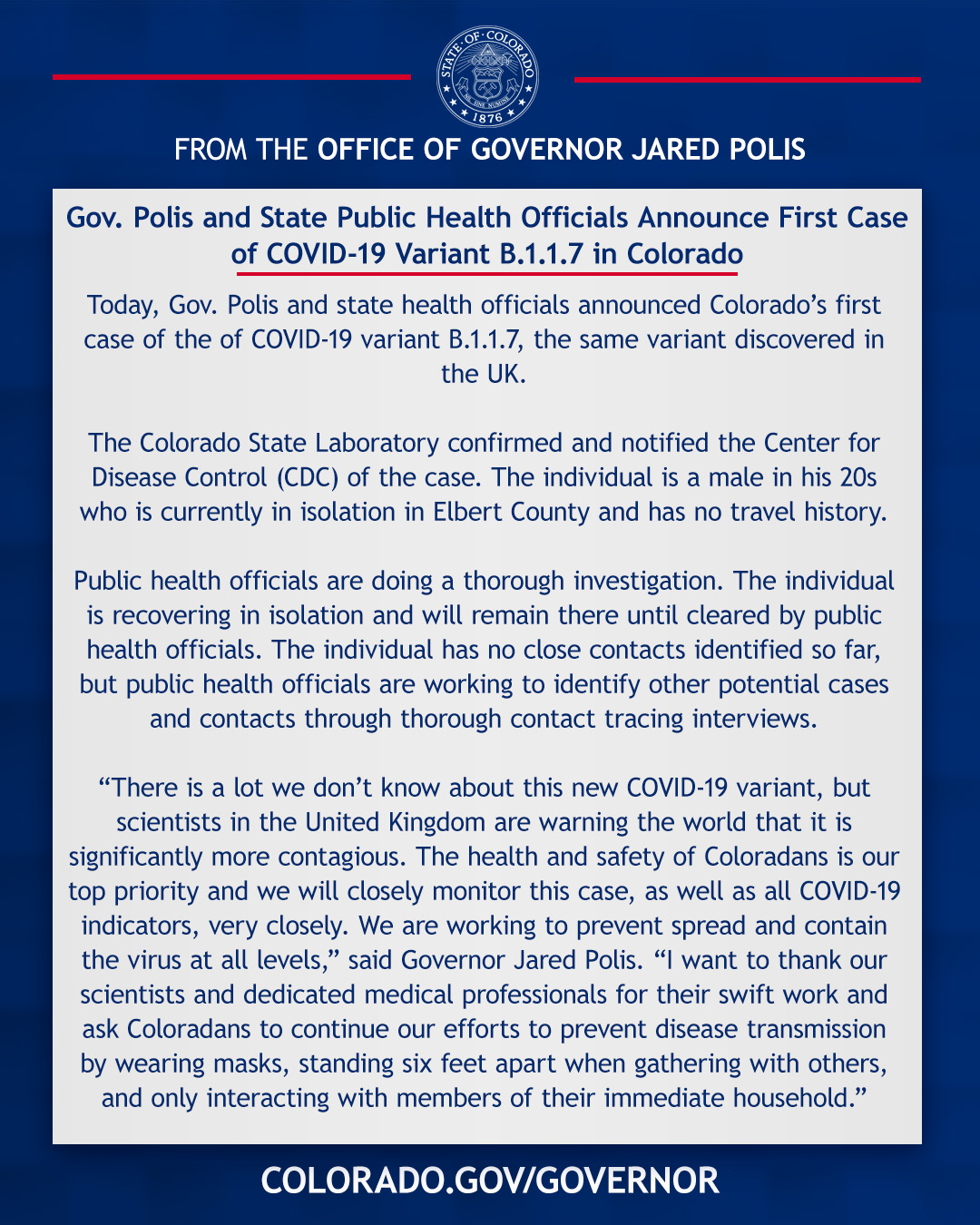
On December 30, the variant was also found in California. This wasn’t unexpected or anything, but finding it in multiple places this quickly is very much not a good sign.
So far I’ve seen two attempts at an estimate. The first comes from CNN. Note this headline’s date for one guess, remembering that the doubling time is plausibly around one week, and the generally conservative nature of such estimates:
It includes this helpful information (as of Dec 22):
Since November 15 — about the time the UK variant might have arrived in the US — genetic sequencing has been done on viruses found in about 300 people in the United States and in about 9,000 in the UK, Worobey said.
So that’s about 60 per week. So we’re looking at about maybe 150 sequences done since the UK made its announcement, and two of them have the new strain?
The other attempt is from Twitter. We have this, from before the California case:
This is the link from that Tweet.
Together with this, again before California:
The implication there is that the above calculations are wrong because the Colorado case wasn’t a random instance of sequencing finding the new strain, rather it was identified another way, so the denominator is unknown.
I do think 50% detection is too high. I don’t know the right way to adjust for the detection method. I also don’t think you can use the month of December as a baseline without a lot of adjustment, since the new strain is suspected of doubling in comparative weight every week not counting imports of new cases, which would also be doubling.
It seems likely we are looking at hundreds or low thousands, perhaps mid thousands, which puts the most likely start of the endgame some time in March if current trends continue and infectiousness is the full amount we suspect.
I think the evidence this past week has strongly favored the new strain being more infectious. What we lack is the knock-down info that would differentiate 50% more infectious from 65% more infectious, to the extent such distinctions are meaningful. My old 70% number may have been premature and therefore somewhat too high, based on others’ evaluations of the same evidence I had at the time, but it now is clearly too low. I’m definitely at least as high as Metaculus, so 90% chance it is 30%+ more infectious, and I’d say 80% chance of 50%+ more infectious.
But What Do We Do Now?
There are, by now, many good faith attempts to think about how likely it is that the new strain is more infectious, or figure out how much more infectious it is. Some of them are in the previous section.
The real problem comes after that. If you are someone who has concluded that the new strain is more infectious, what do you do now? What do you tell people to do?
You have to game out what actually happens from here, and figure out what makes sense and would help, either on an individual level or as a group. I did my best to start that discussion last week, and at least some readers clearly got it.
It seems that everyone who concluded that the new strain is more infectious, but that didn’t directly interact with that post, at least among the people that I can find, instead uses one of two different algorithms
That the new strain is Bad News and Very Concerning, and you should therefore be more concerned and do more prevention, while awaiting more info, like so:
With the more reasonable version of this being “we really really really should do everything to speed up our vaccinations, everyone, and to focus them on those most likely to die of Covid-19.” That’s certainly part of the correct answer, and likely the most important one for us as a group.
On an individual level, however, this is exactly backwards. If you are going to face much more danger in the future than you expected, then that’s a reason to care less about whether you get it now. In the extreme case, if the hospitals may be overloaded in the future while most people get infected at some point, getting it now so you’re immune later might not even be the worst trade.
The other attitude is to exactly echo a year ago, and say there is no cause for concern and try to get people not to “panic” or something. Repeat the messaging of last February, so we can get a repeat of last February. And March and April.
That’s exactly the mistake. If the new strain is much more infectious there, it’s much more infectious everywhere, it will soon be everywhere, and now is the time to worry. Everywhere.
Don’t take his word for it, the WHO is re-running its greatest hit of all:
As Jacob puts it:
So. Yeah.
There’s also this bad take, which I think is bad but which is interestingly wrong, and actually an attempt at a real take, and I do agree with it not being the end of the world:
If we’re doing math, a 50% more infectious strain lowers the herd vulnerability threshold by a third, so if you think we needed 80% before, we’d need 87% now, and the percentage checks out. That’s not the mistake. The mistake is not counting all the extra infections, or the extra extent to which things are ‘hard’ before then if we’re not looking at tons of extra infections, or the way things are hard in other ways if we do get those infections.
In the scenario where our vaccination timeline is a constant and can’t be accelerated, but the control system can somehow adjust infection levels perfectly without inflicting any additional pain, then it’s plausible to say the new variant delays things a month but otherwise changes little. That doesn’t seem plausible to me. If the control system somehow does hold, it means we did a massively expensive crackdown where ‘hard’ is not an adequate description, and one month doesn’t cover it either, since at 5-10% towards an 80%+ target we’d need to be there for half a year or more.
The baseline scenario remains, in my mind, that the variant takes over some time in early spring, the control system kicks in as a function of hospitalizations and deaths so with several weeks lag, and likely it runs out of power before it stabilizes things at all, and we blow past herd immunity relatively quickly combining that with our vaccination efforts.
And yes, I know, I thought early on that either that or suppression would happen last time and I was wrong about it, because I vastly underestimated the power of control systems, and of the two week time horizon of all the politicians, and in general my insufficient amount of cynicism. So it’s quite possible I’m making that same mistake again, and we’re going to make the same mistakes again, even if I can’t actually imagine physically how we pull that off. Nothing is impossible if you have heart. Whatever else you think of these forces, they sure have heart.
Despite that, the conclusion still mostly seems robust, because of several factors. I’ve had a few conversations where it was clear I hadn’t made them sufficiently explicit, so I’ll do that now.
The Control System Acts on Lagged Observations
A fully anticipatory control system wouldn’t have various waves, it would look mostly like straight lines and smooth curves. It’s also not how we observe people talking, acting or reacting, either politicians or private citizens.
Private citizens seem to adjust their behavior to some combination of authoritative messaging, regulatory changes (government interventions), infections, hospitalizations and deaths. Those factors are lagged, and the reaction to them is lagged further still as these reactions are partly accumulative over time and news takes time to travel. Thus, you see waves, often reversing direction quickly once they peak. If you don’t count government restrictions, my model says people are mostly looking at deaths and hospitalizations, with a large share for local anecdotal observations. Their family, their friends, and people they know, and the local hospital, with some role for state and national statistics and news as well.
What happens when the new strain moves in, if it’s fully 65% more infectious (which again means doubling its relative size every week, since each cycle is 5 days)? The growth rate starts to increase slowly, then rapidly. If we index by saying that Week 1 the new strain is 10% of infections and no one’s noticed a change yet, in Week 3 it’s over a third, and in Week 4 it’s the majority. By the time the control system notices the extent of the problem, it’s Week 6-8, and cases are up an order of magnitude or more.
The Control System Is Largely Out of Ammunition
There is no more dakka. I could be wrong about this one, but I don’t see the knobs left to turn that people are still willing to turn. Look at England’s Tier 4, now extended to more areas. I had some harsh words for many of its choices, but do you see them introducing or even seriously considering a Tier 5, or changing their rules to be stricter? I don’t either.
In terms of restrictions, we can’t work any harder than people needing an excuse to be outside. No one will listen, and there’s no way to enforce the rules when they refuse. Even if we could enforce it, the economic and social fallout would be extreme. I can’t even see us having the ability to do this for weeks, let alone months.
In terms of private citizens taking action, there are some people who can be convinced to make one final push to isolate, but those people are being cautious enough already that this change won’t matter much. A lot of the rest of the people are effectively done with and over the whole thing, and I doubt they’d react much at all short of hospital overwhelm. Already hospitals are on the brink, with lots of cases and deaths, and we are seeing the behaviors we see. Good enough for slow improvement, but nothing more than that. Where is the sustained extra 30% cut in risk going to come from?
What we see is a gradual decay in willingness to distance and protect.
We can only work smarter, and I see very little sign we are willing or able to do that. I’d love to be in the world where this new strain causes us to lift restrictions on testing, or on experiments, or even gets us to seriously accelerate vaccinations, and worry more about how fast we go than who gets it first or doesn’t want it. We don’t seem to live in that world, but we might see some movement on vaccination, although I’d expect it only to happen after we see the curves going up quickly again. Given how the timing works, that will be too late.
The Crisis Will Beat the Heat and Outrace the Vaccinations
Another hope is that spring and its warm weather will help to save us, or that we’ll have enough people vaccinated by the time the crisis hits. The vaccinations will help. They might help quite a lot! Nursing homes could be mostly protected, cutting deaths by a third. If we prioritized age after that, we could almost certainly cut down the IFR by more than half before the crisis, perhaps substantially more than that, depending on timing and how much we get our act together.
The problem is that the new strain is already here, detected in multiple states and a lot of countries, so we’re already looking at hundreds of cases minimum. Exponential growth won’t be pretty from there. Unless this isn’t as infectious as it looks, we don’t have the time.
Control System is Reacting to Levels
Along with other factors, people are reacting to current levels of hospitalizations, deaths and infections, in some combination. There is some function that maps from those levels to a level of caution.
In order to stabilize infections, and therefore everything else, we’ll need much stronger reactions than before. In order to get those stronger reactions, and sustain them, we’d need to stabilize at a much higher level of infection than now.
Thus, even if we are in the scenario where we have the ammunition, and we can stabilize, we would stabilize well above 200,000 confirmed infections a day. If we cut the IFR through vaccination, then the control system will notice the relative lack of deaths (and presumably hospitalizations too) and thus stabilize at even more infections than that. That’s the best case scenario.
I think those are the core components of my model that I wasn’t being explicit enough about.
England Approves AstraZeneca Vaccine
This is excellent news, here’s a thread with some details, but hearings weren’t open so we didn’t learn much about their thinking. America should follow suit, but won’t do so any time soon. You see:
Slaoui said that while the AstraZeneca vaccine appears very effective against severe disease, its efficacy among elderly people is “effectively unknown” because few older people were enrolled early in the trial. He said that remains his biggest question about the company’s shot, given the virus’ impact on elderly people.
…
U.S. regulators need more evidence: The drugmaker has said that the combined results showed 70 percent efficacy, but Slaoui suggested that U.S. regulators would not be satisfied by that conclusion.
“As far as the American people are concerned, I think it’s important to say one vaccine has 95 percent efficacy, another vaccine has X percent, whatever that number,” Slaoui told reporters, referring to the high efficacy rates for the Pfizer and BioNTech and Moderna vaccines that the FDA has authorized. “We need a clear and concrete number more than a number that is accumulated by adding together different trials with different schedules and different materials.”
Slaoui also questioned Britain’s dosing strategy. He said it’s possible a booster shot can be more effective when administered months later, but he said that the U.K. decision was based on theory rather evidence.
“It’s important, I think, to use the vaccine based on how you studied it,” he said.
Emphasis mine. The important thing, it seems, is to know the exact value of X.
I would be totally fine given the alternatives, by the way, if we actually are worried about effectiveness in the elderly, with giving the less effective AstraZeneca vaccine to non-healthcare essential workers, who need it less and where we know it will work, while we give the Pfizer and Moderna vaccines to the elderly, almost as if I was trying to solve a physical problem.
If there is one discrete thing that could make a real difference before the new strain hits us, besides actually vaccinating people with what vaccines we have (seriously, can we just pay 10 times as much to the doctors that do it, and if not then show your work), that could still possibly happen, it likely would be getting the AstraZeneca vaccine approved in time to speed things alone. If you have any way to move that needle, please do so, or let us know now to do so.
Two Dose, One Dose, Who Knows, You Knows
As pointed out by many, giving fewer people two doses of vaccine, rather than giving more people one dose of vaccine, when the second option is easier and quicker, and one dose is much more than half as effective as two doses, is rather insane, especially if it means holding half our doses in reserve unused rather than use newly delivered doses for that. Yes, it may make sense to give especially vulnerable or crucial people two doses anyway, but universal two-dosing is hugely destructive.
The good news is there’s considerable movement on this front, despite all the incentives and regulatory barriers.
Canada is doing a non-zero amount of one-dosing, or at least not holding supply back, and letting future deliveries be used for all second doses.
Tony Blair comes out in support of vaccine one dosing. As MR points out, no one is willing to do a cost-benefit analysis, because the result is utterly obvious. The whole point of our regulatory and “ethical” apparatus can be thought of as justification for not doing a cost-benefit analysis. Meanwhile, the one-dose plan is called ‘risky’ because such people think or risk purely in terms of either blameworthiness or in terms of changes from a given baseline scenario. All the people who will die because you two-dosed don’t count towards ‘risk’ in this philosophy, because they’re already going to die, because the ethical guidelines already said that’s what we are going to do, checkmate.
Blair also warns of a future of ‘vaccine passports’ required for travel, with article speculation they could spread to almost everything. I am almost certain such requirements are an almost purely a method of coercion to force people to get vaccinated when they don’t want to, and a means to punish those who refuse. But the requirement sounds so superficially like they’d work as a Sacrifice to the Gods that all opposition seems forced to cite ‘privacy’ concerns rather than raising the question of whether the requirements do anything beyond coercion and punishment. To ask that question, of course, would (among many other things) indicate you are opposed to such coercion.
Only a few days after Blair came out in favor, with every “ethicist” and “expert” calling his proposal crazy as per usual, the United Kingdom is actually doing it. At least to some extent:
This thread has some more details.
There’s also this problem, as always incentives matter:
All I Want For Christmas is a Covid Vaccine, But They Somehow Underpriced Them So Much No One’s Even Bothering To Sell Out
Despite everything, when it came to vaccinating people, I was still insufficiently cynical! The struggle is real.
Your scientists were so preoccupied with whether or not they should, they didn’t stop to think if they could.
Welcome to America’s (and everywhere in the world except maybe Israel’s) Rollout Disaster. We have placed so much emphasis on the priority order, and so little on the logistics and incentives involved and on actually vaccinating anyone at all, that we’re on pace to let many doses sit on the shelves long enough to spoil.
That seems exactly backwards. This reveals priorities.
How is the English vaccination effort going? On the plus side, they’ve approved the Oxford vaccine. That’s super important, and it’s rather terrible that America isn’t following suit.
Otherwise? The way you would expect at this point, similar to America’s, with no sense of urgency.
Again, let’s reveal some priorities:
How about in the United States?
Marginal Revolution reports via this dashboard, As of February 29: Latest CDC vaccine distribution and administration numbers are out.
Doses Distributed: 11,445,175 Doses Administered: 2,127,143 18.6% of the doses distributed have been administered.
Those numbers are even more obviously vastly incomplete than our usual standards, which we know because I have it on very good information (as in, from people who got vaccinated) that the number of vaccinations are happening in places reporting zero vaccinations.
There is one reason for at least some hope, which is that a lot of this could be some combination of Christmas holidays screwing everything up and needing to start things ramping up, and perhaps things will pick up in January, and the slow start won’t end up mattering much so long as not that many doses get spoiled or given to random people to avoid them spoiling:
The video at the source starts with a woman saying, and I quote, “All I want for Christmas is a Covid vaccine” and then she randomly got one. I guess I’ll keep saying it. You never know.
I do think it’s plausible, and we’ll certainly see some amount of pickup in pace, but getting back on track is not the scenario I’m expecting.
Meanwhile, Actual Worst Person Andrew Cuomo has his priorities straight, focusing his fury on those who managed to vaccinate people and threatening not only the doctors involved but the patients who got the vaccine with criminal liability for jumping the line, while most of the doses sit on shelves unused.
But good news, everyone! We are getting ‘coordinators.’
In most places it looks like we haven’t even started letting our actual pharmaceutical distribution system start its work on nursing home residents. We have lots of drug stores. In some places, we plausibly have way too many in ways I’ve been long meaning to explore, so they can hijack business from each other. If we don’t want to let them charge money and also don’t want to pay them, but they still want to do the job anyway as a public service, we could at least let them do their jobs anyway.
So You’ve Decided To Lie to the American People
Dr. Fauci stands out among our most visible health ‘experts’ and officials, and others with influence.
Most talk from such people takes place at Simulacra Level 3+ and is about blame avoidance, group signaling, politics and power.
Dr. Fauci is having none of that, and has firmly made his stand on Simulacra Level 2. His goal at least seems to be to give others a physical model of the world that will cause them to act in a way that makes the physical world better. He also seems to have a meaningfully better grasp of the physical situation, and its gears, than most others who are prominent.
As the one prominent person who is willing to lie to us for our own good rather than lie to us because they are saying the thing one’s political intuition says to say in a situation, he stands as a paragon of relative integrity.
In other ‘better than the alternatives but not exactly the droids we are looking for’ profiles in… something, Kerry notes this quote:
I admit that my first best philosophical sources on which to base public policy are not the criminal protagonists of novels about Mafia families. Despite that, I for one will take arms-length transactionalism over our current standard practices any day.
I leave it as a discussion question what would have happened if Don Coleone was in charge of the pandemic response.
None of this is an ideal situation, and it puts everyone in a tricky spot when he joins 2020 and says the quiet part out loud. Last quote via Marginal Revolution.
Recently, a figure to whom millions of Americans look for guidance — Dr. Anthony S. Fauci, an adviser to both the Trump administration and the incoming Biden administration — has begun incrementally raising his herd-immunity estimate.
In the pandemic’s early days, Dr. Fauci tended to cite the same 60 to 70 percent estimate that most experts did. About a month ago, he began saying “70, 75 percent” in television interviews. And last week, in an interview with CNBC News, he said “75, 80, 85 percent” and “75 to 80-plus percent.”
In a telephone interview the next day, Dr. Fauci acknowledged that he had slowly but deliberately been moving the goal posts. He is doing so, he said, partly based on new science, and partly on his gut feeling that the country is finally ready to hear what he really thinks.
Hard as it may be to hear, he said, he believes that it may take close to 90 percent immunity to bring the virus to a halt — almost as much as is needed to stop a measles outbreak.
Asked about Dr. Fauci’s conclusions, prominent epidemiologists said that he might be proven right…
Dr. Fauci said that weeks ago, he had hesitated to publicly raise his estimate because many Americans seemed hesitant about vaccines, which they would need to accept almost universally in order for the country to achieve herd immunity.
I have no idea if this is smart or dumb messaging, if you disregard the whole lying aspect and the price to be paid for that. It seems like the idea was, we want the maximum amount of prevention, both vaccinations and otherwise. We don’t want to aim too high because then people will despair and give up, and not do enough prevention, but we also don’t want to aim too low because then people will rejoice and not do enough prevention?
My guess is that purely in terms of messaging to get more prevention you want to send the message that the threshold is relatively low. That makes people feel more hope that they can hold out long enough, and makes them feel like taking their vaccine shot helps more? Then of course you can spring on them later the whole ‘herd immunity is non-binary and complex and slow-acting’ thing, or eventually change which definition you’re using.
Claiming close to 90 percent immunity is necessary seems both like terrible messaging, and also not a plausible lie. The number does not make sense. At best it means some super-threshold where you would never see a temporary flare-up.
As lawyers famously ask witnesses, so, were you lying then, or are you lying now? Why should we trust anything you say?
The answer is that he’s both lying and not lying the whole time. He’s saying the answer he thinks will have the best effect on people’s models and thus on their behaviors, in terms of getting them to do the preventative things he wants them to do. That includes a requirement to maintain credibility, and thus not stray too far from what other ‘experts’ say. But beyond that, it doesn’t matter to him what the real number is, and since the definition of herd immunity is (shall we say, see the WHO policy change below) ‘flexible’, it’s not even clear there’s a right or wrong answer here.
Dr. Fauci probably has a true belief for the distribution of possible values for the herd immunity threshold, or at least a best point estimate, but within the range of plausible values for his estimate, that value is not going to impact his stated answer at all. He’s ‘nudging up a bit’ without regard to whether he thinks that makes it more or less accurate.
I do have the instinct that when someone comes out and admits previous lying they’re usually telling the truth about that and their previous statement was the lie, and the current version is more likely to be truthful than the old one. I don’t know if that instinct is good, or whether it applies at all to this case.
To be clear, thank you Dr. Fauci for saying this explicitly. Blatant lies are the best kind! Now, even more than earlier after the whole thing where he and everyone else lied to us about masks, we know what we are dealing with. But it’s a bad look, ya know? And if anything you seem proud of the whole idea rather than treating it as regretful while arguing it was necessary, or something similar.
Which leads to reactions like this:
The W.H.O. is also playing fast and loose with herd immunity, here’s a good catch by CarellaJoe:
In June, you were immune no matter why you were immune. In November, only immunity from the vaccine counts.
This matters. The consequences include vaccinating people who are already immune because they’ve already had Covid-19. Including still giving them priority, and even making it mandatory for many of them, and then giving them an even more useless second vaccine dose.
In general, the new definition is less useful and fails to cut reality at its joints. This is not where to draw the boundaries. The new one was chosen in order to drive rhetoric.
In light of all that, here’s an interview of Dr. Fauci on Podcast-19 in which he delivers his message. How much of it to believe is up to you. There isn’t any concrete new info here. His response to the new English strain is, of course, reassurance combined with general need for concern, but he was only asked about its impact on vaccinations.
Vaccine Allocation By Politics and Power
You expected allocation via politics and power to mostly be fair, and you never thought the leopards would eat your face, aw, that’s cute:
Essential sectors like… finance.
I am not as curious about this one as Olivia.
Here’s New York’s priority list, which looks relatively sane and fair given the decision to kill off a bunch of old people:
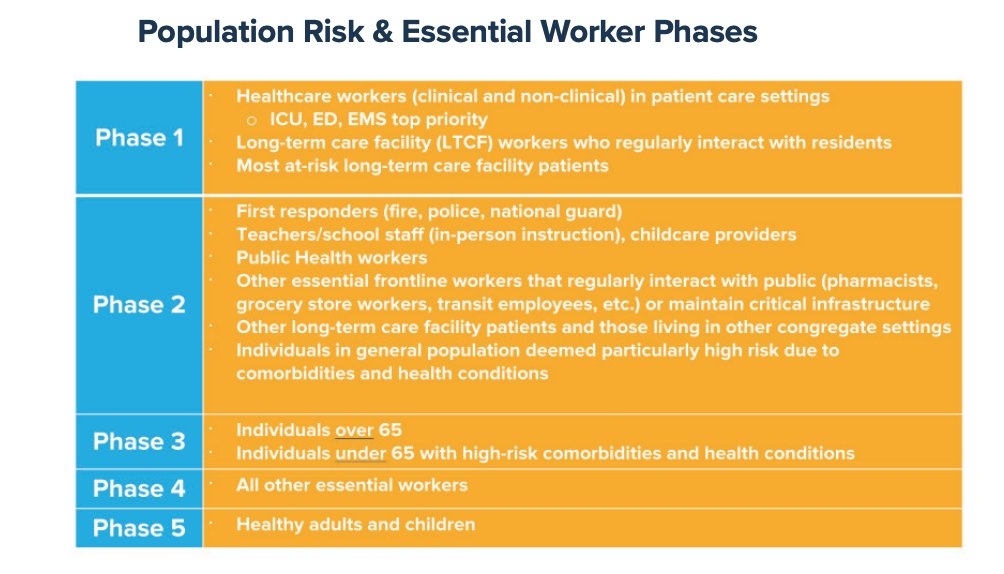
Expect a lot of very interesting definitions of both ‘regular interaction with the public’ and ‘essential’ in the coming months.
Also, here’s one part of how Cuomo is interpreting that order in practice:
There are plausible utility functions where addicts in rehab could get relatively high priority, but I am confident they are not anything the public would take kindly to let alone endorse or see as “fair.”
Each of those dots is in order of priority so expect massive delays as we pause to clear each step before starting the next one.
Even when you do offer the vaccine to the right people, they’re not the ones who want it…
Also worth noting that if you have two reasons to vaccinate someone first, increased risk of infection (whether or not only virtuous risk counts) and increased risk of death given infection, you might consider doing the obvious, and you could even shut up and multiply to get risk of death.
Complexity is bad, but we’re doing other complex things in the name of politics and power, so if we’re doing both of these things anyway then there’s much less excuse for not even mentioning this option.
Via this twitter thread, more detail on how the CDC decided that racial ‘equity’ was important enough to choose plans that killed more people rather than less people. As a reminder, the argument is that elderly people are disproportionately white, so giving the vaccine to elderly people first is racist.
If you oppose such priorities, it does not seem that we are out of the woods on this:
Marcella Nunez-Smith, a co-chair of Joe Biden’s COVID-19 advisory board, commended the experts at the CDC for “taking political interference out of the process” and for “their grounding in inequity.”
In addition to the central argument that it’s better to kill more people so that deaths are distributed ‘equitably’, there’s this gem that’s worth pondering:
One graphic from Oliver’s presentation, used to illustrate the trade-offs of prioritizing the elderly, cites a statement from the American Geriatric Society that “age should never be used to exclude someone from a standard of care, nor should age ‘cut-offs’ be used” to allocate scarce supplies. It also notes that the Health and Human Services Office for Civil Rights had objected to triaging ventilators by age at the start of the pandemic.
Regardless of how you value ‘equity’ versus ‘people not dying’ it is interesting to decide for yourself whether this is an immensely dishonest use of that quote, or if it is instead completely fair.
Obviously the American Geriatric Society was arguing against discrimination against the elderly. The quote was originally in the context of ventilator allocation.
But what is the principle here?
Is it exactly what was said, that “age should never be used to exclude someone from a standard of care, nor should age ‘cut-offs’ be used to allocate scarce supplies?”
Or is this one of those one-sided anti-discrimination principles, where you can never favor young over old for any reason, but you can favor old over young all you want? There do seem to be a bunch of these going around lately. In general, if one wants to say that you can favor group X over group Y, but never group Y over group X, you should say that, rather than say “never favor one group over another group.”
In the spirit of blatant lies are the best kind, and rewarding the creation of clarity, I do want to thank the advocates of such policies for their honesty and transparency. Whatever else one might think of such priorities, they had the courage to openly admit what they were, and not to attempt to fudge the predictions that such actions would result in more people dying. And also they did not pretend they were deciding on some other ethical principle or practical advantage, despite reasonable arguments being available. They could have said that those out there volunteering to take risk deserve our protection, or had considerations of efficiency and reliability of service provision, the same way that it’s a great relief to know that the health care workers are vaccinated when you yourself might need their care. Instead, they went with their true objection. We should applaud that.
In other vaccines allocated via power and politics news, did you know that if you pay very little money for something, you often get less of it?
I am a physician in private practice in [redacted]. We have just been approved to order and administer the vaccine to tier-appropriate patients. Medicare has approved a payment of 18$ for the first shot and 28$ for the second. As far as we can determine we will not be allowed to bill for an office visit so that is the entire amount we will receive for registering the patients, screening then for covid outside of the office, taking their vital signs, taking a history to see if there are any contraindications to the vaccine, administering the vaccine, observing them in the clinic for a minimum of 15 minutes up to 30 minutes depending on their history, and recalling them in 28 days and going through most of the same procedure again, minus the registration and history. There is also an extensive regime of recording and reporting all vaccination data daily to the state government. We had anticipated hiring someone to manage this new service due to the amount of new work that is required. At this rate we might be able to give 10 shots an hour in each of our 3 clinics if we see no other patients for illness, injury, or covid testing.
Do I need to say that we cannot possibly afford to do this for the reimbursement offered. The alternative is for patients to receive the vaccine in some state funded site or clinic. That may take a very long time to roll out.
It’s one thing to not charge the patient. I get that. But to not sustainably compensate the doctor? What was the plan here?
Israel has a better plan, which includes: Vaccinate 24⁄7:
Health Minister Yuli Edelstein called Thursday to keep the vaccine operation going 24 hours a day, 7 days a week, including on Shabbat.
Regarding the push to carry out vaccinations on Shabbat, Edelstein, who is Orthodox, cited the Jewish legal principle of saving a life, or “pikuah nefesh,” which trumps nearly all other religious requirements.
According to a Channel 12 report Saturday, Clalit, Israel’s largest health maintenance organization, will open 24⁄7 vaccination centers in Tel Aviv, Haifa and Herzliya in the coming days to help ramp up the pace of the vaccine drive. Additional centers are expected to be opened at a later date.
Israeli hospitals are also to join the vaccination effort next week, and hundreds of IDF medics will also participate, to help expedite the process.
For comparison, NYC vaccinations by day, where the city that never sleeps seems to at least be snoozing every so often:
One country thinks saving lives is the highest obligation of us all, including as a religious obligation. The other pays forty-six bucks and forbids charging anything additional.
If you don’t like allocation by politics and power, and you don’t want to allocate by willingness to pay, you can always take door number three, and allocate as Florida is doing among the elderly via willingness to stand in line. This way, instead of money being transferred, the competition is about who is willing to destroy the most value (via standing in a line that could get people infected, in the middle of winter, for many hours). It also means that the more vulnerable you are, the harder it is to get vaccinated.
Still, Florida is prioritizing the elderly over the non-elderly, and prioritizing those willing to send a costly signal over those unwilling to send such a signal. I’m guessing this is still an upgrade over the realistic alternatives. I’d have been tempted to use this thing called ‘appointments’ but that would slow things down, and it’s plausible that even a small speed boost is more important than everything else. So overall, give my regards once again to Governor DeSantos.
There are always good arguments about people in charge not having that much control over events, but I still think Democracy works better when we give people the right incentives even if it means some unfair evaluations, and fully endorse this, adjusted for degree of difficulty:
From Bloomberg, 3 million doses known to be delivered as of morning of 12/31:
In Other News
Good Twitter thread from Youyang Gu of Covid Machine Learning Projections about why he thinks the CDC’s estimate that 100 million people in the USA were infected by December 1 is mistaken. Lots of meat to get into here and it’s the holidays, so I’m deciding not to have time for this week, but I hope to revisit next week.
If you’re wondering what the FDA was doing instead of approving Covid-19 vaccines, it was fighting the good fight against Bucatini, which is essentially spaghetti with a hole in it. At first it looked like this was because with all the restrictions and shortages people were using Bucatini as straws, but it’s a pre-cooked food and the FDA was worried this was unsafe and therefore put a hold on the product. But it turns out, it’s nothing as fun as that, it’s merely that the EU and USA have distinct requirements for the enrichment of flour and a rival pasta company tipped off the FDA that the pasta was meeting the wrong requirements, in order to gain a business advantage over their rival. Whether that’s a better or worse look for anyone involved is an open question.
But that’s not all. The FDA was also hard at work charging $14,060 fees for distilleries that produced badly needed hand sanitizer. Because now they are ‘drug manufacturing facilities.’ They take their status as President of the Delenda Est Club seriously.
Washington Post piece on our early failures to provide a Covid-19 test, which Thailand deployed within 1 day, and which took any given private citizen 1 day with ordinary skill in the art plus any kind of lab to work with, but took the CDC 46 days while we banned all private efforts (Twitter HT).
Yet another way we could test for Covid-19 and catch it before people become infectious, if that kind of thing were legal. They’re getting it approved to monitor insulin continuously, which is highly useful. Offhand, they mention that oh by the way it can detect a ton of other things too, including Covid-19.
Imperial College in the UK is finally doing a challenge trial starting in January (hurray!) with results in May. Far too little, far too late, but it’s still a bargain at ten times the price, and hopefully it makes it easier to do such things next time.
Completely inessential and off-topic, but too good a headline to not share: Game Of Thrones Showrunners’ New Netflix Series On Hold After Suspected Murder.
Matt Yglesias offers words of wisdom on the failures of our messaging about masks and other preventative measures, and especially how the early emphasis on dirty surfaces continues to focus people on all the wrong things. Even knowing surfaces don’t matter and telling people over and over surfaces don’t matter and knowing we all still pay too much attention to surfaces, I still pay too much attention to surfaces.
I’ve said it before so You Should Know This Already, but a periodic reminder that the UK was paying people specifically for people to dine in at restaurants is still worthwhile. Did you know that people got to use the discount a fixed number of times, but it could be used on a dining party of any size?
Yes, the systems involved really are this perverse.
While some of us have been effectively put under house arrest by the pandemic (see the rest of the linked thread) this is your periodic reminder of how seriously many regular folk who think they are being responsible took all of this:
California’s pandemic response, summed up in one Tweet:
Good thing we are extending the order that few are following and that no one is enforcing. This is what passes these days for ‘rule of law.’
Off-topic spoiler-free review of Tenet: Four out of five stars, made perfect sense, ask me anything. But not here.
Conclusion
I want to thank everyone who took my warnings of last week seriously, and helped spread the word. We got a shout-out in Shtetl-Optimized, as he offers his “crackpot theory” that if we were a functional civilization we might have acted like one and vaccinated everyone a while ago. Also all those who looked into the information available, and decided for themselves how likely the new strain was to be various levels of infectious. What we most need more eyes and thoughts on, regarding the new strain, is figuring out how all of this plays out, and what we might do to change the outcome, either collectively or individually.
It is super tricky to reason through the implications of the current situation. I still don’t know if one should buy stocks, sell stocks or do nothing. It’s not even obvious if one should be focused on taking more or less precautions. And I don’t see any careful thinking about the hardest part for me to figure out, which is what authorities are likely to do and how we might shift their thinking. I do not see people wrestling much with these questions.
We also have a vaccination crisis. WIth the new strain coming, getting as many people vaccinated as fast as possible becomes that much more important. Instead, we will be giving up on AstraZeneca until April, and are so bad at putting shots into arms now that we need to be worried about doses spoiling. Even after everything, I didn’t consider that we would botch things that badly. I figured it would cost lives if we administered vaccines later than we needed to, but supply would still mostly be the limiting factor, so mostly only supply would matter. Surely we wouldn’t be so terrible at this that we’d throw out millions of doses.
And yet, here we are, and that has become a distinct possibility. Hopefully it will not come to pass, but it will have come scarily close. All we have to do is offer reasonable compensation to those tasked with putting shots into arms, and give those people shots to put into arms. At this point, I don’t even care that much which arms the shots get put into, relative to getting those shots into some arms rather than no arms.
If you know about any way at all to move that needle, please at least let others know how to do so.
Few things would make me happier than to be wrong about all this.
Finally, arbitrary cutoffs like December 31 still matter. Virtual party at the walled garden.I wish all of you a Happy New Year, whose first six months are nothing like the new year I expect. Whether or not the pandemic will be over soon, good riddance to 2020 is one thing we can all agree upon.
If anyone knows how to use money to speed up vaccine delivery I’d love to know. I might be able to quickly allocate something like $5-20M but I have no idea who to work with to do it. CA would be easiest. Also easier if it’s in a poor community like the central valley but honestly any leads would help.
Were you able to find a lead?
I live in Southern England and so have a fair bit of personal investment in all this, but I’ll try to be objective. My first reaction, upon reading the LSHTM paper that you referred to, is ‘we can no longer win, but we can lose less’ - i.e. we are all headed for herd immunity one way or another by mid-year, but we can still do a lot to protect people. That would have been my headline—it’s over for suppression and elimination, but ‘it’s over’ isn’t quite right. Your initial reaction was different:
You give multiple reasons to expect this, all of which make complete sense—Lockdown fatigue, the inefficiency of prevention, lags in control systems, control systems can’t compensate etc. I could give similar reasons to expect the alternative—mainly that the MNM predicts the extreme strength of control systems and that it looks like many places in Europe/Australia did take Rt down to 0.6 or even below!
But luckily, none of that is necessary.
I would encourage everyone to look at the scenarios in this paper since they neatly explain exactly what we’re facing and mean we don’t have to rely on guestimate models and inference about behaviour changes. This model is likely highly robust—it successfully predicted the course of the UK’s previous lockdown, with whatever compliance we had then. They simply updated it by putting in the increased infectiousness of the new variant. Since that last lockdown was very recent, compliance isn’t going to be wildly different, weather was cold during the previous lockdown, schools were open etc. The estimate for the increase in R given in this paper seems to be the same as that given by other groups e.g. Imperial College.
So what does the paper imply? Essentially a Level 4 lockdown (median estimate) flattens out case growth but with schools closed a L4 lockdown causes cases to decline a bit (page 10). 10x-ing the vaccination rate from 200,000 to 2 million reduces the overall numbers of deaths by more than half (page 11). And they only model a one-month lockdown, but that still makes a significant difference to overall deaths (page 11). We managed 500k vaccinations the first week, and it dropped a bit the second week, but with first-doses first and the Oxford/AZ vaccine it should increase again and land somewhere between those two scenarios. Who knows where? For the US, the fundamental situation may look like the first model—no lockdowns at all, so have a look.
(Also of note is that the peak demand on the medical system even in the bad scenarios with a level 4 lockdown and schools open is less than 1.5x what was seen during the first peak. That’s certainly enough to boost the IFR and could be described as ‘healthcare system collapse’, since it means surge capacity being used, healthcare workers being wildly overstretched, but to my mind ‘collapse’ refers to demand that exceeds supply by many multiples such that most people can’t get any proper care at all—as was talked about in late feb/early march.)
(Edit: the level of accuracy of the LSHTM model should become clear in a week or two)
The nature of our situation now is such that every day of delay and every extra vaccinated person makes us incrementally better off.
This is a simpler situation than before—before we had the option of suppression, which is all-or-nothing—either you get R under 1 or you don’t. The race condition that we’re in now, where short lockdowns that temporarily hold off the virus buy us useful time, and speeding up vaccination increases herd immunity and decreases deaths and slackens the burden on the medical system, is a straightforward fight by comparison. You just do whatever you can to beat it back and vaccinate as fast as you can.
Now, I don’t think you really disagree with me here, except about some minor factual details (I reckon your pre-existing intuitions about what ‘Level 4 lockdown’ would be capable of doing are different to mine), and you mention the extreme urgency of speeding up vaccine rollout often,
But if I were writing this, my loud headline message would not have been ‘It’s over’, because none of this is over, many decisions still matter. It’s only ‘over’ for the possibility of long term suppression.
*****
There’s also the much broader point—the ‘what, precisely, is wrong with us’ question. This is very interesting and complex and deserves a long discussion of its own. I might write one at some point. I’m just giving some initial thoughts here, partly a very delayed response to your reply to me 2 weeks ago (https://www.lesswrong.com/posts/Rvzdi8RS9Bda5aLt2/covid-12-17-the-first-dose?commentId=QvYbhxS2DL4GDB6hF). I think we have a hard-to-place disagreement about some of the ultimate causes of our coronavirus failures.
He’s totally right on the facts, of course. The question is what to blame. I think our disagreement here, as revealed in our last discussion, is interesting. The first order answer is institutional sclerosis, inability to properly do expected value reasoning and respond rapidly to new evidence. We all agree on that and all see the problem. You said to me,
Implying, as you’ve said elsewhere, that the malaise has a deeper source. When I said “2020 values” I referred to our overall greater valuation of human life, while you took it to refer to our tendency to interfere with private action—something you clearly think is deeply connected to the values we (individuals and governments) hold today.
I see a long term shift towards a greater valuation of life that has been mostly positive, and some other cause producing a terrible outcome from coronavirus in western countries, and you see a value shift towards higher S levels that has caused the bad outcomes from coronavirus and other bad things.
This is probably the crux. I don’t think we tend to go to higher simulacra levels now, compared to decades ago. I think it’s always been quite prevalent, and has been roughly constant through history. While signalling explanations definitely tell us a lot about particular failings, they can’t explain the reason things are worse now in certain ways, compared to before. The difference isn’t because of the perennial problem of pervasive signalling. It has more to do with economic stagnation and not enough state capacity. These flaws mean useful action gets replaced by useless action, and allow more room for wasteful signalling.
As one point in favour of this model, I think it’s worth noting that the historical comparisons aren’t ever to us actually succeeding at dealing with pandemics in the past, but to things like “WWII-style” efforts—i.e. thinking that if we could just do x as well as we once did y then things would have been a lot better.
This implies that if you made an institution analogous to e.g. the weapons researchers of WW2 and the governments that funded them, or NASA in the 1960s, without copy-pasting 1940s/1960s society wholesale, the outcome would have been better. To me that suggests it’s institution design that’s the culprit, not this more ethereal value drift or increase in overall simulacra levels. There are other independent reasons to think the value shift has been mostly good, ones I talked about in my last post.
As a corollary, I also think that your mistaken predictions in the past—that we’d give up on suppression or that the control system would fizzle out, are related to this. If you think we operate at higher S levels than in the past, you’d be more inclined to think we’ll sooner or later sleepwalk into a disaster. If you think there is a strong, consistent, S1 drag away from disaster, as I argued way back here, you’d expect strong control system effects that seem surprisingly immune to ‘fatigue’.
Many of the same thoughts were in my mind when I linked when I linked that study on the previous post.
----
IMO, it would help clarify arguments about the “control system” a lot to write down the ideas in some quantitative form.
As I wrote here:
Even a simple toy model could help, by separating intuitions about the mechanism from those about outcomes. If someone argues that a number will be 1000x or 0.001x the value the toy model would predict, that suggests either
(a) the number is wrong or
(b) the toy model missed some important factor with a huge influence over the conclusions one draws
Either (a) or (b) would be interesting to learn.
----
One basic question I don’t feel I have the answer to: do we know anything about how powerful the control system is?
Roughly, “the control system” is an explanation for the fact that R stays very close to 1 in many areas. It oscillates up and down, but it never gets anywhere near as low as 0, or anywhere near as high as the uncontrolled value of ~4.5.
As long as this trend holds, it’s like we’re watching the temperature of my room when I’ve got the thermostat set to 70F. Sure enough, the temperature stays close to 70F.
This tells you nothing about the maximum power of my heating system. In colder temperatures, it’d need to work harder, and at some low enough temperature T, it wouldn’t be able to sustain 70F inside. But we can’t tell what that cutoff T is until we reach it. “The indoor temperature right now oscillates around 70F” doesn’t tell you anything about T.
Doesn’t this argument work just as well for the “control system”? A toy model could answer that question.
I agree, and in fact the main point I was getting at with my initial comment is that in the two areas I talked about—namely the control system and the overall explanation for failure, there’s an unfortunate tendency to toss out quantitative arguments or even detailed models of the world and instead resort to intuitions and qualitative arguments—and then it has a tendency to turn into a referendum on your personal opinions about human nature and the human condition, which isn’t that useful for predicting anything. You can see this in how the predictions panned out—as was pointed out by some anonymous commenter, control system ‘running out of power’ arguments generally haven’t been that predictively accurate when it comes to these questions.
The rule-of-thumb that I’ve used—the Morituri Nolumus Mori effect—has fared somewhat better than the ‘control system will run out of steam sooner or later’ rule-of-thumb, both when I wrote that post and since. The MNM tends to predict last-minute myopic decisions that mostly avoid the worst outcomes, while the ‘out of steam’ explanation led people to predict that social distancing would mostly be over by now. But neither is a proper quantitative model.
In terms of actually giving some quantitative rigour to this question—it’s not easy. I made an effort in my old post, by saying how far a society can stray from a control system equilibrium is indicated by how low they managed to get Rt—but the ‘gold standard’ is to just work off model projections trained on already existing data like I tried to do.
As to the second question—overall explanation, there is some data to work off of, but not much. We know that preexisting measures of state capacity don’t predict covid response effectiveness, which along with other evidence suggests the ‘institutional schlerosis’ hypothesis I referred to in my original post. Once again, I think that a clear mechanism - ‘institutional sclerosis as part of the great stagnation’ - is a much better starting point for unravelling all this than the ‘simulacra levels are higher now’ perspective that I see a lot around here. That claim is too abstract to easily falsify or derive genuine in-advance predictions.
I’m trying to think through how “increase in R” interacts with population heterogeneity (a frequent theme of this newsletter, but not mentioned in this particular one!)
This is me thinking out loud. Following is some paragraphs of math which readers can skip, my conclusions are in the last two paragraphs.
Imagine a histogram of everyone in a city. The horizontal axis is “how many microcovids of exposure does this person get per week?” but normalized to (i.e. divided by) the prevailing COVID rate in the city. The vertical axis is “fraction of the population” (again, this is a histogram). Heterogeneity means that the histogram is spread out—some people are almost completely isolated (a peak around 0) while others are out partying, way far to the right.
Actually, let’s omit all the immune people from our histogram. So OK, now there are a lot fewer people way out on the right, because most those people have caught COVID already. There are still some people way out on the right, either because they’ve been lucky, or because they recently jumped rightward—having run out of ability or willingness to isolate as much as before.
Call that histogram H.
Now multiply H by “a line through the origin with slope 1” (y=x). That gives us a function F(x) = x · H(x). While H had a big peak of hardcore isolators on the left side (near 0 microcovids / week), F mostly doesn’t have that peak, it got squashed down by the other factor. Conversely, out on the right, the curve for F is pulled way up, relative to H.
The area under F is proportional to R, the reproduction number.
Now what?
Herd immunity would look like reducing the area under H, which in turn reduces the area under F. Remember, immune people don’t get included in H. Vaccines would push down all parts of H, whereas community spread would disproportionately push down the right part of H, which has a bigger impact on F per person.
Lockdowns would look like squeezing H leftwards, which then reduces the area under F.
Now, let’s say it’s November 2020 in some USA city, and R just jumped up from 0.9 to 1.1. What’s the story? There are different possibilities. One story could be: everyone uniformly increased their microcovids by 20%. We grabbed the H curve and stretched it to the right, like a rubber band. Another story could be: 1% of the population just said “f*** it” and increased their microcovids by 2,000%. A new peak appears in H, way off to the right, pulling weight from elsewhere. The consequences of these two stories are different. In the first story, we need maybe 5-15% of the population to get infected (or 20% to get vaccinated) to get back to R=0.9. In the second story, just that 1% will quickly get infected and immune, and then we’re rapidly back at R=0.9.
Now we learn that, under current conditions, the new strain is, let’s say, 1.65× as infectious as the old strain. So we know that the area under F increased by 1.65×. The simplest story would be: every person has 1.65× as much microcovids as before (again, I mean “microcovids normalized to the prevailing infection rate”). That’s not quite true, but I suspect it’s close enough. So the new strain has stretched H horizontally, pulling it rightward by a factor of 1.65 (and squished it vertically to keep the same area under it). As usual, we have community spread pulling weight disproportionately out of the right side of H, and vaccinations pulling weight more uniformly out of H. How does it play out? I dunno, it’s kinda hard to say.
So where are we at? There’s a subset of people in the USA that are still almost completely isolated, including (in my narrow experience) a subset of New York Times liberals and Bernie progressives, a subset of people with serious comorbidies who can work from home or are retired, etc. They’re still way out on the left, not contributing any appreciable weight to F (i.e., they’re not contributing to the community spread = R). If their microcovids go up by 1.65×, well, they will still not really be contributing any weight to F. Then there is a big tail of other non-immune people with progressively more exposure, who constitute the bulk of community spread. If their microcovids go up by 1.65×, well, a lot of those people will catch COVID-19 who otherwise wouldn’t, before the area under F shrinks below 1 and cases start going down.
So if you compare March-April 2021 (in cities where the new strain has caught fire) to November 2020, say, we have 1.65× more exposure holding behavior fixed, but on the other hand, we’re talking about the behavior about the 50-70th percentile least isolated people (say), instead of the 70-90th percentile, because the latter already caught it in November-January. I don’t have a good sense for how those balance out, but it doesn’t seem so crazy to me to propose that a late-spring peak would be comparable to the peak we’re in now, as opposed to much larger. Maybe each peak infects 20% of the population, or something? I don’t really know, I just made that number up. But if we wind up with 50% infected at the end, well, I think I have a decent shot at not being one of those 50%, and it would make sense to keep trying...
My current main selfish takeaway from this is that given the new strain and likely properties of it, I and my loved ones will likely get infected (whereas in the previous world I estimated our precautions as sufficient to prevent infection.)
Hence my main thoughts turn to treatment. I am currently acting on the recommendations provided in the link Zvi previously posted (https://www.quora.com/What-is-the-current-treatment-for-Covid-19) - I would love if anyone has better next actions specifically re treatment than those listed in the Quora response.
to add to the advice on metformin: berberine has a similar mechanism of action (relevant for COVID: AMPK) and is available OTC.
Metformin has a rare but dangerous side effect called lactic acidosis. This side effect is much more likely to happen if you are acutely unwell or have a serious infection.
Zvi, I still think that your model of vaccination ordering is wrong, and that the best read of the data is that frontline essential workers should be very highly prioritized from a DALY / deaths averted perspective. I left this comment on the last thread that explains my reasoning in detail, looking at both of the published papers I’ve seen that model vaccine ordering: link. I’d be happy to elaborate on it but I haven’t yet seen anyone provide any disagreement.
More minor, but regarding rehab facilities, from a bureaucratic perspective they are “congregate living facilities” and in the same category as retirement homes. I don’t think New York is doing anything exceptional by having them high on the list, for instance California is doing the same thing if I understand correctly. We can of course argue over whether it’s good for them to be high on the list; I personally think of them as 20-person group houses and so feel reasonably good prioritizing them highly, though I’m not confident in that conclusion.
I read people claiming that the first doses first strategy could cause evolution of the virus to escape the vaccine. Is there any truth to that? Does that factor into the cost-benefit analysis?
(From this retweet from a Prof at Geneva Centre for Emerging Viral Diseases)
Does not make that much intuitive sense to me because there are a lot of random mutations happening. If the first dose first (or first dose only) strategy reduces the size of the whole SARS-CoV-2 viriome, there will be fewer viruses and less genetic variation in total. More infections in total means more genetic diversity. More infections means that a vaccinated person will be exposed to more sources of infection, more virions, more different genomes over time, thus also increasing the likelihood of mutants able to escape the immunologic response.
Does that assume that the amount of mutations (and therefore the risk of an immune escape) is only dependent on the size of the viriome? But isn’t it possible that the risk of an immune escape mutation in the 1-dose vaccinated population is much higher than in the rest of the population? I think if that was much higher, it could swamp the benefit of reduced overall chance for dangerous mutations occurring due to the reduced infections from vaccinating more people (as compared to 2 doses). Not sure of any of this, just trying to think through your intuition.
A follow up thought: What do we know or what can we guess about the effect of 1-dose on reducing transmissibility? If we vaccinate twice as many, but they are still very much infectious (compared to 2-dose), could that be a problem?
The WHO redefinition part looked weird to me, so I tried to verify it. The 13 November text verifies at the Internet Archive—though note that the text shown in the screenshot is only the beginning of the entry. The entry contained many more paragraphs of text, but I don’t see it correcting the weird definition of “herd immunity” that it establishes at the beginning.
However, the current text as I am seeing it live on 31 December (last update today, apparently) is significantly different; it gives a lot of space to the benefits of vaccination, but does not phrase it in such a way as to ignore other immunity sources the way the 13 November text did, and makes it clearer that the “herd immunity through vaccination” is a normative claim on actions that should be taken and not a positive or nominative claim on what herd immunity actually is. Here’s the current first paragraph, emphasis mine:
The rest of the new text more or less matches this change from the 13 November version; there is a bit about “The fraction of the population that must be vaccinated against COVID-19 to begin inducing herd immunity is not known”, but that’s several paragraphs in and I read it as pretty well-contextualized to “given that the plan is to vaccinate until we reach that point”. Here’s the first sentence from the third paragraph, emphasis mine:
The part I emphasized in that sentence is actually identical in the 13 November text, but badly contextualized. (The other differences in the third paragraph are immaterial to the distinction under question, consisting only of additional explanatory text—I assume to help readers who don’t have a basic gears-model of immune response and viral transmission readily in memory.)
Importantly, and to restate something from above, the third and all subsequent paragraphs are missing from the right-hand screenshot in the post, and it doesn’t look like normal truncation at a glance—the whitespace at the bottom of the screenshot visually implies that the second paragraph was the end of the entry in that version, which is false.
IA snapshots show that the 13 November text was in place up through 27 December, so perhaps not a small blip in terms of Internet time, but it does seem to have been corrected.
I was not able to verify the 9 June text, since IA shows no snapshots of this URL before October. I imagine perhaps the URL was different, and I would appreciate a hard reference if anyone has one.
About the English strain part. This seems very one-sided to me. Only the evidence in favor of it being more infectious is being shared by Zvi.
In Denmark 12.5% of all positive COVID are randomly sequenced. The English strain has been observed in the samples since 14 November. However it remains stable at 0.5-1% of samples. This makes me update in the direction that it is not 70% more infectious compared to other strains. Otherwise we should see the strain make up a larger proportion of positive samples over time. (https://files.ssi.dk/engelsk_virusvariant-28122020)
The graph “One of these lines on that second graph is not like the others” is highly selective. You can add other European countries with a similar slope as UK where the English strain is not responsible.
I don’t think it’s correct to say that it remains stable at 0.5-1% of samples in Denmark. There were 13 samples of the new variant last week, vs. only 3 two weeks ago, if I understood the data correctly. If it went from 0.5% to 1% in a week then you should be alarmed. (Although 3 and 13 are both small enough that it’s hard to compute a growth rate, but it certainly seems consistent with the UK data to me.)
I think better evidence against non-infectiousness would be Italy and Israel, where the variant seems to be dominant but there isn’t runaway growth. But:
- Italy was on a downtick and then imposed a stronger lockdown, yet the downtick switched to being flat. So R does seem to have increased in Italy.
- Israel is vaccinating everyone fairly quickly right now.
At the time of writing the weekly percentages were 0.3%, 0%, 0.2%, 0.5%, 0.9% which I did not perceive as weekly doubling. But I was likely fooled by the noise of the first weeks where numbers were too low to be meaningful. Yesterday latest weekly numbers came out and last week the percentage was 2.3%. So numbers are clearly worrying and in line with Zvi’s post.
Do you have a source for B.1.1.7 being dominant in Italy/Israel?
Assuming it’s already dominant there, that strongly suggests that it’s infectious enough to have rapidly outcompeted other strains, but that Italy/Israel were able to push down the higher R through some combination of behavioral change and vaccination.
(Note: I can’t find any sources saying B.1.1.7 is dominant in Italy or Israel, and I’d be surprised if that were already the case.)
See here: https://cov-lineages.org/global_report.html
I might be missing something, but where in this link do you see the dominance? If it is the large proportion of sequencing showing B.1.1.7 (18/33 for Italy and 4⁄13 for Israel), isn’t that due to increased surveillance, like testing positive people coming from the UK?
You may well be right. I guess we don’t really know what the sampling bias is (it would have to be pretty strongly skewed towards incoming UK cases though to get to a majority, since the UK itself was near 50%).
Is there any chance that block quotes could be formatted as such?
This is probably just a problem with the import
I also thought that, but it’s like that on his blog also.
Three days ago, nearly the same day Zvi posted this, it was announced that Israel will stop vaccination between Jan. 10th and Feb. 1st, because there are not enough doses. During these three weeks, all available doses will be used to give people their second shots.
While the lack of doses is not the Israeli government’s fault, this was surely foreseeable; not communicating this earlier (before Jan 30th) will further reduce confidence in the government. When vaccinations resume, I expect people to fight more over their place in line, because they’ll be afraid of another pause.
The option of delaying the second dose has been proposed; so far the politicians seem to be against it. Also, one of our higher ranking doctors came out against it with a wonderful quote (idem, emphasis mine):
It’s a good thing Zvi only manages the Delenda Est club for the US, or it would take up most of his posts.
Some numbers: as of yesterday (Jan 2nd), we have vaccinated 1.09 million people, 12.59% of the population. The average vaccination rate for the past week (27.12-03.01) was 81,200 vaccinations per day (more on weekdays, less on the weekend). If this continues for another week, we’ll have vaccinated 1.65 million people, or 19% of the population, with a single dose. A good start, and perhaps enough to make a significant change in outcome for the vulnerable populations who were vaccinated, but I assume it’s far from enough to drive R below 1.
Disclosure: I am Israeli, and in a prioritized category (chronic illness). I received my first dose of the Pfizer vaccine on 1.1.2021.
Good news. On January 10th it was reported we got another vaccine shipment from Pfizer and are back on track to vaccinate everyone over 16 years old by the end of March, and hopefully to continue lowering the minimum age after that to 12 or below. Vaccination is now open to everyone over 55 years old.
Renegade Option:
1. Get a list of trusted contacts from the rationalist network in each state
2. For each state,
* Determine where vaccines were sent.
- Find the number for the State Department of Health.
- Call and ask about the distribution of vaccines. Who would have the list?
- If this fails, compile a list of local hospitals/pharmacies to call and ask if they have received vaccines.
* Get contacts in state good enough PPE to just show up and interact with strangers
- order KN95s and faceshields to their door
- buy a head air bubble to lend out to people for a cause like this.
3. Find the number of a good lawyer. Learn how to give shots and use an epipen.
4. For areas local to our contacts,
* Stand in a public spot with a clipboard + form asking for names and fast contact method of people interested in getting contacted in the event we successfully manage to get excess vaccines. Collect risk categories or bids as well if interest seems high enough to warrant prioritization.
* Compile a list of local hospitals/pharmacies.
* Call and ask if they have received vaccines, and what they intend to do if they have more vaccine than they can use within the time or patient groups they have. If our ad hoc list would benefit them in creating such a plan.
* Buy syringes as needed, and a good cold box. Also an epipen and some OTC anti-inflammatories.
* Call or show up at pharmacies about to close up with offer to distribute any extra sitting around.
- Probably don’t phrase this as “take the trash out for ya” and wink exaggeratedly if you can help it.
* Take a picture at pharmacy to support provenance.
* Call people in FIFO order (or 2nd price bid plus a couple random pro bono picks) and tell them to hightail it to their new appointment time at a park (or more probably outside your house since we’re gonna want to keep vials very cool.)
* Jab them. Keep watch for 10-30min in case they have an allergic reaction.
Now. What does the non-renegade version of this look like?
Basic question about the two-dose one-dose cost-benefit analysis:
What is the prior to have on how soon you need the second dose to confer long-term immunity? The data we have is on 3 weeks between dose 1 and 2, and that shows 92% immunity reached with the single dose, but now it sounds like e.g. the UK is gonna hold back that second dose for some amount of time, and I can imagine that being like 2 months or so. Anyone know how long is too long?
Reasoning by analogy, via some googling:
Here is how it works for the MMR vaccine (measles, mumps, and rubella):
Or here are the WHO recommendations for various vaccines (from the larger source here) for children. The times in the Booster Dose column span months or years. This doesn’t quite answer the question of how soon you need to be, but does provide an intuition for the orders of magnitude which are typically involved, at least for children. Though besides age, I suppose part of the epidemiological reasoning here must involve not just the reaction of the immune system, but also the prevalence of the disease.
(just throwing it out there) Since this is our second year with covid, maybe we can make a more informed effort to prevent other maladies to lessen the overall strain? I mean, on the individual level.
We used to have a baseline for how sick we become and when to more or less expect it (chronic or seasonal things) and/or how often Shit Happens (accidents). We might want to adjust it.
It used to be ok, to look for something for the pollen allergy in the spring or in the fall, but if one already knows one will need it later, why not buy it now? If there’s a vegetable garden one is too old to tend alone, then plan around the need to invite more people to do it*.
Father Frost brought me a new toster :) I thought “oral contraceptives in bulk” were kinda not his thing. Now I think I was wrong.
*where I live this would be a sacrilege. Lots of people come greet their neighbors when the time to plant potatoes strikes again.
ChristianKI just wrote about the need to not overdo the more physically demanding tasks after isolation.