BA.2 became the majority strain in the United States this week, as expected. Mostly things are continuing as expected, with unsurprising news on a variety of fronts. The biggest surprise is that the second booster shot was approved. Given I expect to be asked about that every so often, I split that off into its own post.
Executive Summary
BA.2 now majority strain but for now it changes nothing.
Ultraviolet light confirmed as effective.
Lack of federal pandemic funding having real world impacts.
Second booster approved for those 50+ or who are immunocompromised.
Let’s run the numbers.
The Numbers
Predictions
Prediction from last week: 177k cases (unchanged) and 6,200 deaths (-12%).
Results: 189k cases (+6%) and 5,718 deaths (-18%).
Prediction for next week: 210k cases (+11%) and 5,100 deaths (-10%).
Looking back, I didn’t adjust for Colorado backfilling some deaths last week, which likely explains why there was a bigger than expected drop this week.
For next week, as BA.2 takes over I expect case growth to accelerate somewhat, but continue to not expect things to get terribly out of hand before stabilizing once again. That could still take a month or two to happen.
Deaths
Death numbers continue to decline as previous masses of cases work their way out of the ‘counts as a Covid death’ window. The blue bump is Colorado’s backfill last week.
Cases
NYC cases, make sure to use a log scale edition. The uptick isn’t not worrying but I do not expect it to be sustained for that long, and as Zeynep says previous infections should ensure that even relatively bad scenarios do not get so bad.
BA.2 outlook, wastewater in Boston ticking up from low baseline.
In UK, ZOE study claims record high case numbers, but official numbers are dropping and well below peak. Who is right?

Yes, tests are down, but how much?
How does that translate in percentage terms?
The positive test rate is slightly higher than the January peak. This implies that a somewhat smaller percentage of cases are being caught. It does not plausibly indicate that the rate of finding cases has declined by more than half.
Physical World Modeling
CDC has BA.2 becoming 55% of cases for the week ending March 29, up from 35%.
Vaccine effectiveness data for BA.2 has come in. Meet the new vaccine effectiveness, same as the old vaccine effectiveness.
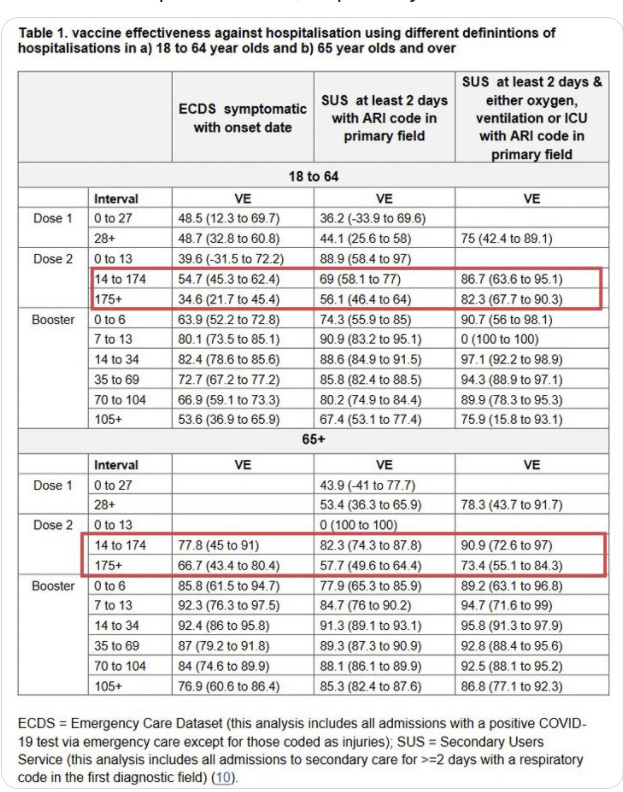
Additional new CDC vaccine efficiency data for the Omicron wave.
There is nothing here for 1 or 2 mRNA doses alone, but I’d assume 2 mRNA doses to be between 2 J&J doses and the 3-dose regimen that includes J&J.
The RECOVERY trial: A randomized controlled trial for the win. Still ongoing.
And now, a new experimental treatment is looking promising, thanks to a similar study called TOGETHER.
Last week, a clinical trial called TOGETHER produced two potentially important conclusions: A little-discussed experimental drug called peginterferon lambda cut in half the number of Covid-19 patients who ended up going to the emergency room or hospital. And the much-discussed antiparasitic drug ivermectin failed to prevent hospitalization for Covid patients at all.
TOGETHER, like the RECOVERY study conducted in the United Kingdom and REMAP-CAP, conducted basically everywhere but the United States, was a platform study, a streamlined clinical trial that evaluated multiple medicines at once and that use a common placebo group. It’s from these platform studies that doctors have learned perhaps the most about Covid-19.
…
“The only trials that have given us useful information during the pandemic have been the platform trials,” Mills told STAT in an interview, also citing the PRINCIPLE trial, which showed an inhaled steroid could reduce complications, and the PANORAMIC trial, which is starting in India.
It looks like the handful of players in the greater people-who-think-and-care-about-what-works then move-fast-and-break-things ecosystem somehow are the only ones other than major corporations who get much done anymore:
But there’s no arguing these small trials, which were comparatively inexpensive, delivered huge amounts of information. RECOVERY cost less than $10 million. Mills said the budget for TOGETHER was also $10 million. And it didn’t come from the National Institutes of Health, a big drug company, or a major charity.
Instead, one of the major funders of the trial so far has been Patrick Collison, co-founder of payments firm Stripe, who Forbes estimates to have a $9.5 billion fortune. New funds are coming from the charitable foundation FTX, a cryptocurrency exchange, and its founder Sam Bankman-Fried, who is worth $24 billion, also per Forbes.
“One of the big questions is where are the big players in this?” asked Mills. “Where is Gates Foundation? Where is NIH? Where is Wellcome Trust?”
Where are they indeed? About here.
“I think pre-pandemic nobody knew how badly organized medical research is, and we assumed the esteemed investigators and big name universities or NIH would have systems in place about how to move rapidly,” Mills said. “It turns out they didn’t.”
Fluvoxamine and caffeine do not mix well. Unless you want very long lasting caffeine and damn the consequences, in which case maybe they mix awesomely? Not my area.
New Vitamin D study finds that giving people with low D concentrations Vitamin D pills does not prevent Covid, with doses tested up to 3,200 IUs a day which should have been sufficient. There was no sign of extra adverse events.
Self-reported adherence to study supplements among participants randomized to either intervention arm was good, with 90.9% of participants reporting that they took study supplements at least 6 times per week.
In the subset of participants included in the intention-to-treat analysis for whom measures of end-study vitamin D status was available, mean 25(OH)D concentrations were significantly elevated in the higher-dose vs. no offer group (102.9 vs. 66.6 nmol/L respectively; mean difference 36.3 nmol/L, 95% CI 32.9 to 39.6 nmol/L), and in the lower-dose vs. no offer group (79.4 vs. 66.6 nmol/L respectively; mean difference 12.7 nmol/L, 95% CI 9.8 to 15.6 nmol/L; Table 2, Fig. 2).
So it does look like there was at least some actual Vitamin D involved. One hypothesis they tested here is whether offering people free and convenient Vitamin D can cause people to take the Vitamin D, and the answer seems to mostly be yes. But also, even mentioning it seems like a strong intervention in terms of uptake:
On the other hand, another subset (49.9%) of participants randomized to no offer took a vitamin D supplement on one or more occasions during follow-up.
This may have led to increases in 25(OH)D concentrations in the no offer arm over the course of the study, although seasonal effects (sampling in June vs. December) will also have contributed.
This is compared to (via quick Google) 28% of Americans who take Vitamin D supplements. They note here that D concentrations did rise in the control group.
One potential hypothesis is that many or most gains are from fixing extreme deficiencies, and by testing everyone they got those with extreme deficiencies taking Vitamin D even if they were in the control group. This still does seem reasonably robust. Taking Vitamin D seems to clearly be a ‘free action’ as there were no negative effects, and there are lots of people who are deficient (e.g. Google says 42% of Americans are deficient) but this seems less urgent. I will continue to take it, but I have updated.
Bob Wachter asks what the immunocompromised should do, and notices how much his model says one can reduce their risk.
He also reminds us about Evushield, which I haven’t talked about, but which is a big help to immunocompromised people.
Look at the risk reductions here. 90%+ decline incases. 90%+ decline from masking (which seems very generous unless it’s a super-mask, but they do exist.) Additional benefit from Omicron, he says 25% and I think it’s far more than that. Then 80% or more from Paxlovid, again I think that’s on the low end. That’s three orders of magnitude, and you get another one from vaccination. There’s various light cheating involved here, but we’re talking three orders of magnitude from an at-most single-digit baseline.
Those reductions mostly also apply to everyone else.
I strongly agree with the conclusion. Things are not going to get meaningfully safer than they currently are. Life is short, especially when you are in poor health. Live it.
Doing More
Biden says do no more, or at least do not let Covid control our lives.
I agree strongly. Others disagree. They say to Do More.
Doing More. Doing More, like war, never changes.
Here’s a standardized call this week to Do More.
Here are some vaccination statistics, therefore we must do more.
That first number is pretty awesome. We got 97% of those over 50 to take the first shot. That second number is also pretty great. We got 84% fully vaccinated. I am still confused by there being far more people who declined the second shot than the first shot, but the other 16% are likely going to be impossible to get.
The third number, that only about half are boosted, is not as good. But how are you going to ensure that they get more protection? There has already been plenty of opportunity, and a lot of people do not want the third shot. I think they are making a mistake, but I see no shot at convincing them.
The fourth shot is both a lot less worthwhile than the third shot, and also where most of our remaining ‘more’ comes from at this point. Of those who are most vulnerable and who got third shots, a lot of them will presumably opt for fourth shots, and this will provide substantial additional protection for some number of months. My guess is it has about zero effect long term. Whether that is worthwhile for them is their decision, and will depend on the future path of the pandemic, but we can only do what we can do.
Here is some advice to ‘not try and time’ the fourth shot. That seems obviously silly to me. The whole idea on additional shots is a short burst of protection, and exponential growth happens over the course of weeks or months but the booster takes a week to work. So yes, absolutely it seems easy, provided the decision to get another booster at all, to usefully time one’s additional boosters. Same source also says to hold off if you’ve had Covid in the last three months, which very much seems automatic.
Biden’s budget includes over $80 billion in pandemic funding, including a 171% increase in funding for the CDC. The White House explicitly reminded us that such budgets are statements of principle, as Congress has the power of the purse. And is currently refusing to use that power on much, so it seems highly unlikely we will see very much of this money allocated. It is a dilemma when an organization like the CDC fails so utterly. Do you use this as evidence that it needs more funding, or that it has no ability to use funds well and should if anything get less? Ideally one starts over from scratch, or at least seriously reforms. I don’t see any signs of that.
Look at all the things we have shortages of when everything is fine, they say.
This makes such claims have no meaning. If we are always in shortage of such basic items no matter what, even when everything is fine, then I can’t take such complaints as having any meaning. That does not mean we aren’t in trouble if there is a ‘surge’ from BA.2, but health care would eat actual everything if given the chance.
Prevention and Prevention Prevention Prevention
White House is continuing to push air quality, a welcome development, perhaps partly motivated by their lack of funding for doing anything else while previous stimulus that mostly had nothing to do with anything health-related could be used to upgrade air filtration. Words of wisdom:
“It’s important that this becomes a passive control measure — passive in the sense that it doesn’t require people to do anything,” said Joseph Allen, director of the Healthy Buildings program at Harvard University’s T.H. Chan School of Public Health. “It’s not requiring you to wear a mask, or wear a good mask or wear it right. It’s operating in the background all the time.”
Article emphasizes the amount most of the top public health authorities actively sabotaged efforts to improve air quality by flat out denying its impact for most of the pandemic. For example:
The CDC in October 2020 first acknowledged “limited, uncommon circumstances” when people were infected with the virus through airborne transmission, particularly in enclosed spaces with inadequate ventilation. Later, in May 2021, the agency revised its guidance to emphasize that airborne transmission was a significant driver of infection.
I saw no mention of legal requirements. The last thing I want is to make it that much harder to build, and that much more expensive to live and have buildings, but we should be encouraging those with the ability to do so to improve ventilation.
In addition to air quality, another neglected front is ultraviolet light, which I have also been largely neglecting. A new paper suggests that it is highly effective at prevention (direct link), to strength previously existing evidence.
For context, this is effectively an order of magnitude improvement.
They decline to note particular commercial devices, but yes they are available. I expect almost no one to purchase them, but they are at least being used a non-zero amount (MR).
PCR tests will now cost the uninsured $125, Congress did not step in and prevent this.
Japan reaches a compromise that seems tough but fair.

China
Scott Gottlieb once again on television to point out that China is in quite the pickle. They ‘will have a hard time containing this’ he says, which is quite the understatement.
Something is wrong with OurWorldInData’s China numbers, as BNO News is reporting very different and much bigger numbers and other sources back them up. So do the numerous reports of how zero Covid no longer looks sustainable, and also various financial market moves that people are explaining as coming from the disruptions expected in China.
The new center is Shanghai, one of the world’s biggest cities. I’ve speculated that China had little spare capacity to conduct operations, and also that it was not all that committed to success like it used to be, and here we have confirmation of both (next day data link).
Shanghai is divided by a river, so they’re going to lock down the first half, test it, then lock down the second half and test there. As I remarked at the time this seems certain to be both unnecessary and insufficient. It is not part of any plan designed to achieve zero Covid. Rather, it is part of a plan that signifies the doing of things.
While the lockdown is in place it is hardcore. No one is allowed outside at all. There are robot dogs patrolling the streets. Those who want their non-robot dogs to go outside may resort to drastic measures (2 minute video).
These are flashes of the ‘do whatever it takes’ attitude, but without willingness and ability to sustain such restrictions and costs across China, it will still not be enough.
Perhaps a miracle will somehow occur. I do not expect one.
Think of the Children
Or, don’t, because you don’t have to. No news here very much is good news.
In Other News
No, seriously, no one cares about Covid anymore.
I am somewhat concerned Russia/Ukraine is not considered more urgent than this, but inflation seems like a very reasonable top concern.
Looking back on Ivermectin and its early studies.
Here is the full interview of David Redmond I asked about a few weeks ago. He is hugely overconfident, both at the time and in hindsight, but there is much wisdom in his perspective. Putting people like him in charge would be a large improvement.
“The FDA is now selling indulgences” is not fair, when over $100 million dollars is paid to get a rapid FDA decision it’s not the FDA that is selling.
Telemedicine abortion becomes permanent in UK after surprise vote. Seems great to have more permanent telemedicine available, although this seems like an ‘odd flex’ to do on its own.
In India, they are extending approval of their homegrown vaccine Corbevax to children without data to support that. More than the usual suspects are unhappy.
I do agree that ‘zero public data’ is not a sufficient amount of public data to make a decision on whether to require something. I do think it’s totally fine when deciding whether to allow something, provided we are capable of making that distinction. If parents and children want to take the vaccine without data backing it up, they should be able to make that choice, so long as everyone understands the choice being made.
I don’t know the extent to which India is capable of that.
The complaints about favoritism, regulatory capture, corruption and double standards, on the other hand, seem spot on. If you are going to have a general principle of Right to Try, and let people make their own choices, that’s great. I salute that principle. If you’re only going to do that for the political favorites, not so much.
Making this about vaccine inequality seems exactly backwards to me. This is a general pattern when addressing inequality.
One group X has access to more and better than another group Y.
To address this, we ban the thing group Y has access to for ‘equality.’
Now some of group Y gets what Xs have, but most group Ys have nothing.
It would be better if everyone in the world had access to mRNA vaccines at no charge. Assuming we cannot get this first-best solution, ‘equality’ demands we be more generous allowing others to access what vaccines they can get, not less, the same way that banning ‘not good enough’ housing or child care or anything else simply means prices go up and often the poor end up going without.
We do those in need no favors, whether as individuals or as countries, by doing this. One can say ‘poorer countries deserve no worse than rich countries’ but as long as they remain poorer trade-offs will remain a thing. Also, usually imposing such restrictions hurts everyone, rich or poor. One could turn this around, and say that everyone deserves not to be physically prevented from taking life saving medicine whether they live in a poor country or a rich one.
Once again there is the issue of ‘trust.’ Once again, trust is framed as whether health experts can express trust. Nice vaccination program you have there. Shame if some health experts were to… lose trust in it. Very alarming. Better give what we ask.
Would I give this vaccine to my children if I lived in India and had no access to an mRNA vaccine? I likely would not do so without further research. I can imagine getting to the point where I thought this was net positive based on public information. I can also imagine looking and not getting there.
Not Covid
IRB Review, when do you need it?
Interacting with humans is not an inherently dangerous action. Making it in the context of ‘research’ or ‘medicine’ does not make it so. Until we change this, the war on knowing things will continue.
Eliezer Yudkowsky asks, can someone actually defend frequentism for real, and make a worthwhile case that Bayesianism is meaningless?
The learning I found here is that there are a bunch of people suggesting someone else can provide a defense, but the actual provided defenses do not seem to fulfill the requirements. The search for a robust and eloquent frequentist continues.
Fascinating stuff about possible beneficial effect of MMR and TDAP boosters—they could help mitigate the risk of getting Covid:
https://www.sciencedaily.com/releases/2021/08/210831142423.htm
Re your question about whether the Zoe or official numbers are likely to be correct in the UK.
It seems likely that it’s Zoe, based on other data and on the physical situation.
The other data source is the Office for National Statistics. They’ve been running a sampling study, going out and testing the population. They are finding very high levels of infection. It’s about 1 in 16, or 3.4 million people in England who would have tested positive a week or two back. (Plus some more for Scotland, Wales and Northern Ireland.) That seems very compatible with Zoe saying 340k cases per day across the whole UK.
https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/bulletins/coronaviruscovid19infectionsurveypilot/latest
The relevant information about how things are going is that there has been a massive change in testing. People in the UK used to be able to request a free pack of 7 lateral flow tests to be delivered by post every day. As of today, those are no longer available. Officially, over the last few weeks you could still order them every 3 days, but in practice they have been almost completely out of stock.
The guidance and general tone has also changed, with much less attention to COVID in general and on testing in particular.
Given that tests are so much less available, it’s almost surprising that as many cases are being detected as are.
Agree with this, though I wouldn’t trust ZOE numbers going forwards.
https://twitter.com/PaulMainwood/status/1509563756644286464 this is the mostuseful estimate I know of at the moment (comparing the ONS survey, case numbers adjusted based on the ONS survey to compensate for ascertainment, and ZOE) - note that ZOE has generally been unreliable since Omicron, but it does nevertheless seem to be true that cases are currently higher than the January peak.
On China: apparently Our World in Data was only reporting symptomatic cases for consistency with earlier in the pandemic, but almost all of China’s positive tests were asymptomatic (see https://twitter.com/PaulMainwood/status/1509069309011808256)
As nuts as IRBs can be, their purpose is not to protect people from research findings but from research (mis)conduct. They are to protect the human subjects.
Misconduct of gain-of-function research (i.e. leaking a plague) might harm people. So might research misconduct for nuclear weapons (blowing people up, irradiating a water supply) and world-changing AI (grey goo / insert your favorite scenario). The most you can say is that IRBs are for protecting human subjects selected for the research from harm, and the above research types don’t select any human subjects (even though they implicitly might affect any nearby civilians and possibly the whole world). I would call that “technically correct: the best kind of correct”.
Tl;dr;
You don’t need a frequentist. Get someone who fulfills some criteria like:
Thinks likelihood functions are a bad idea
or are unnecessary to do science
can explain how they’ll fail
Thinks the issue lies elsewhere. (A den of thieves cannot be made honest merely through the introduction of p-values, likelihood functions, or any other mathematical construct which does not _)**
“In order to do probability you must understand the domain. Part of science is exploring.”
** It’s a social issue not a technological issue. Or:
It’s a tech/knowledge issue not a math function issue.
-
(The thing itself)
It’d be funny if someone read that and said ‘no serious frequentist takes p-values seriously’. Seriously though, I can imagine someone dismissing both p-values and likelihood functions.
“So you want to figure out if a study is good or not, using just one number.
It doesn’t work. Go home. Or learn how to do science so you can do your job.”
(“But why can’t we just calculate-”
“Statistical power? You could try using that. But something tells me you won’t. It’s just a hunch I got, after I noticed that fact that you frequently cite studies that people have tried to replicate. Tried, and failed. But hey, correlation isn’t causation, all we know is that one happened before the other. They could be completely unrelated.”)
Is this just the U.S.? Like the wastewater thing? Or is it widespread? Is it ongoing supply chain issues?
What do you think about the intra-lung UVA treatment?
Huh. I was going to say that “warning, UVC is dangerous. It’s not ‘neglected’, it’s evaluated and discarded for very good reasons”.
And then I started digging.
The main issues with UV are: 1) eye damage, 2) skin damage, and 3) ozone production.
Turns out that there’s apparently surprisingly recent research showing filtering out wavelengths longer than 230nm helps significantly with 1[1] and 2[2], which is weird. I would normally expect shorter wavelengths to be more destructive. (Hypothesis is that the shorter wavelengths have a lower penetration distance, and so ‘just’ kill cells that are on the surface and going to be shed shortly anyway?)
And there’s apparently a window around ~220nm that’s short-wavelength enough that it avoids 1⁄2, but long-wavelength enough that it doesn’t have significant ozone production[3]. And KrCl lamps peak at 222nm.
Yet another small update in favor of tuned physics, I suppose. (Small update. There are many possible combinations of a few elements + power to produce EM radiation.)
That being said, I’d be much more relaxed if the paper had explicitly monitored/measured room O3 concentration, and/or if they had also filtered out short wavelengths.
https://pubmed.ncbi.nlm.nih.gov/33749837/ (...in rats)
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8638665/ (in human, singular)
Although that being said, many common UV lamps also produce ozone due to arcing[4]. This component can largely be mitigated by proper design.
https://onlinelibrary.wiley.com/doi/pdf/10.1111/php.13391 - though take it with a grain of salt, as it’s by someone that produces UVC lamps.
Regarding more people declining the second shot than the first shot, my best guess would be that people took the first shot, and either they themselves or one of their acquaintances had an extremely bad side effect, either actual or perceived, so they decided not to take the second shot. I know one person who followed this reasoning. Her husband fell ill after his vaccination with unclear causes, and she attributed it to the vaccine. She finally did decide to get her second shot and booster recently.
Another possibility could be that some financial incentives incentivized the first shot but not the second shot.