The new year is about to start out with a bang.
For five weeks, we’ve seen Omicron double and double again. That which can’t go on forever, won’t. There aren’t many doublings left. This is it.
The CDC’s revised guidelines made it even more clear that we’re going to collectively make the right decision, let it happen, and hope for the best. It’s not like we have any choice in the matter.
A month from now, we’ll be on the way back down, and we’ll know how bad it was and what the death toll will end up looking like.
Two or three months from now, if all goes well, The After Times can begin in earnest after all the previous false starts.
Executive Summary
Cases way up despite holiday, and will keep going up.
Testing is increasingly difficult to get.
Too early to know if hospitals will be able to handle it.
See Omicron Posts (#10 from Tuesday) for further details.
Let’s run the numbers.
The Numbers
Predictions
Prediction from last week: 1.85mm cases (+80%) and 10,200 deaths (+10%).
Results: 1.81mm cases (+77%) and 8,599 deaths (-6%).
Prediction for next week: 3.5mm cases (+94%) and 10,800 deaths (+25%).
Note that some other sources have more cases than Wikipedia for the past week (e.g. BNO reports the total case count as closer to 2.1mm).
With how much things are changing each day and how many confounders there are, getting the case count that close was largely luck.
What will happen this coming week?
Uncertainty is through the roof on that, except that it will be a lot higher as we enter fog of war. Testing capacity will be exhausted and thresholds to get tested will rise in some places while desperation to get tested pre-emptively rises in others. It’s possible a few places like NYC will peak, while others haven’t fully taken off yet. On top of it all, we don’t know how much the holiday ended up slowing things down, and how much of what’s happening the past few days is filling in a backlog, so we don’t know what the right baseline is.
I’m going to go with an average of 500k cases per day, for 3.5mm total. I wouldn’t be that surprised to miss high by up to a third, or miss low by quite a bit if things are still doubling every few days and we manage to identify enough of those cases.
This is it.
On deaths, it looks like the West and Midwest are still on vacation in terms of reporting deaths, and it’s not obvious they’re going to fix this by next week. Which means they might backfill those deaths (which would count and not be corrected) or they might continue not to report. This assumes they’ll probably at least report the correct share, but it’s hard to tell.
Deaths
Tennessee had a giant backlog dump, of which I’ve substracted 1,800. We don’t get to add in all the obviously missed deaths in the West and Midwest, so I missed high here.

What we’re seeing here is still Delta combined with holiday reporting. It will take another two weeks before we have much color on the real death rate going forward. Three weeks to be sure.
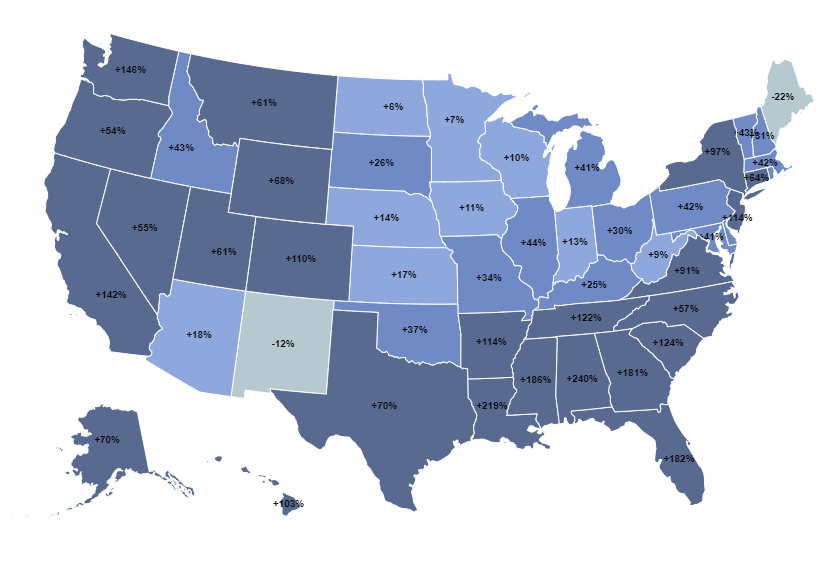
Cases
Also this handy map that updates in real time.

One way to estimate the true rate of cases is to look at the rate of incidental Covid-19, which is the positive test rate of a random sample. People who land in the hospital for non-Covid reasons aren’t the most random of samples, but they’re also not the least random either? Plus, if you have a baseline, you can control for the bias in the sample (in both directions) by comparing similar populations.
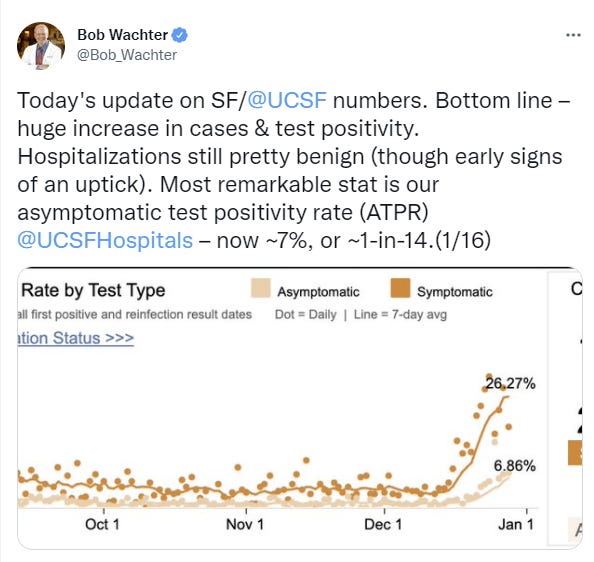
I was about to kick myself for not getting onto this method of analysis earlier, except that it’s not available anywhere else?
Vaccine Effectiveness
Canadian data shows vaccines have been super effective, a 20x reduction in deaths, but that was prior to Omicron.
You know what we still never got anywhere on settling, and which is super relevant right about now? The extent to which vaccines make some people immune to infection while others largely aren’t, versus the extent to which they make most people less vulnerable to infection in each encounter but not fully immune.
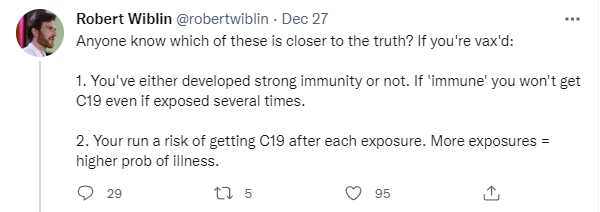
This has always been important, but Omicron makes it even more central. If it’s fully option one, then it makes sense at this point to be essentially fully all-or-nothing (or a-lot-or-not-much, at least) on risks once you’re boosted. Either you’re immune and you’ll be fine, or you’re not immune and you were never avoiding Omicron anyway, it wasn’t worth it. If it’s fully option two, paying more attention to marginal risks is justified.
My model now says it’s a hybrid. People have different levels of antibody and other responses to the vaccines, which means some people are effectively fully immune (at least for a while), others get more limited protections, and you get some Bayesian evidence over time for where you stand based on how much risk you take and whether you get infected.
Vaccination and Vaccine Mandates
If you’ve declined to be vaccinated, you’re also likely going to decline to take Paxlovid.
Of those who were familiar with the Pfizer pill, the poll found 84% are likely to take it if they test positive for the coronavirus, with no large differences between generations, racial groups, or political affiliations.
But there was one key difference: 91% of vaccinated people would take the pill, but only 52% of all unvaccinated Americans said they are very or somewhat likely to do do so. The likelihood an unvaccinated person would take the pill dropped even further — to 35% — among those who said they would never get vaccinated, compared to unvaccinated people who said they will “wait and see.”
That’s a huge correlation. I’ve seen some grasping at straws that Paxlovid might somehow be dangerous, but mostly everyone agrees it’s great and it’s not at all a political issue. So this suggests the vaccine hesitancy largely isn’t about politics or any concrete concerns either. Half the people who aren’t vaccinated have sufficiently strong priors against doing anything new that they’re having none of it, it all sounds super suspicious to them, and you’re not going to tell them different. The alternative hypothesis, which I find less plausible, is that the political divide carries over to everything else automatically at this point, which is functionally the same but has some different implications.
I notice I’m not sad about it. It’s a scarce treatment, so if some people don’t want it, there are plenty of others that do.
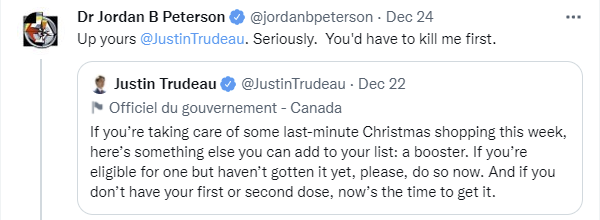
Justin Trudeau’s attitude here seems like exactly what one would want, politely asking citizens to do the thing he believes is best. So, a proportionate response would be… give me liberty, or give me death?
That doesn’t mean that the mandates we have are wise or reasonable or make any sense as prevention as opposed to punishment. If your mandates don’t start going into effect until January 15, and they ramp up in March, what’s the point? I don’t expect it to be ‘over’ by then but the peak would have already at least be close.
(Editorial link, it’s standard stuff.)

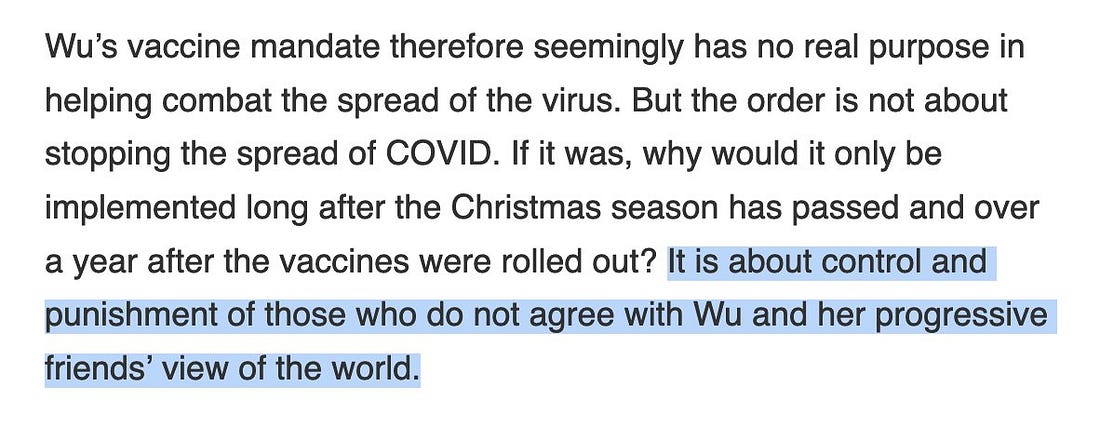
I do think that the similar original NYC mandates were (at least in part) object-level attempts to accomplish something. I don’t think anything imposed going forward can make that claim.
Also, sometimes you don’t have enough workers so you don’t enforce your vaccine mandate to avoid shutting down services, you can just say that, except no, you can’t say that, so you pretend bus drivers are isolated from the public.
CDC Revised Guidelines Continued
I wrote a post yesterday about the CDC’s revised guidelines on how long to isolate if you test positive for Covid-19. The story very much continues, so consider this a Part 2.
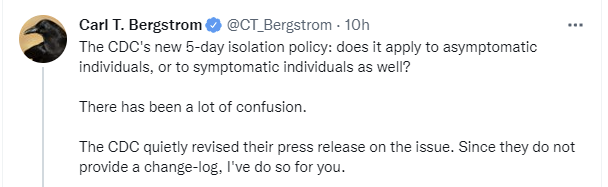
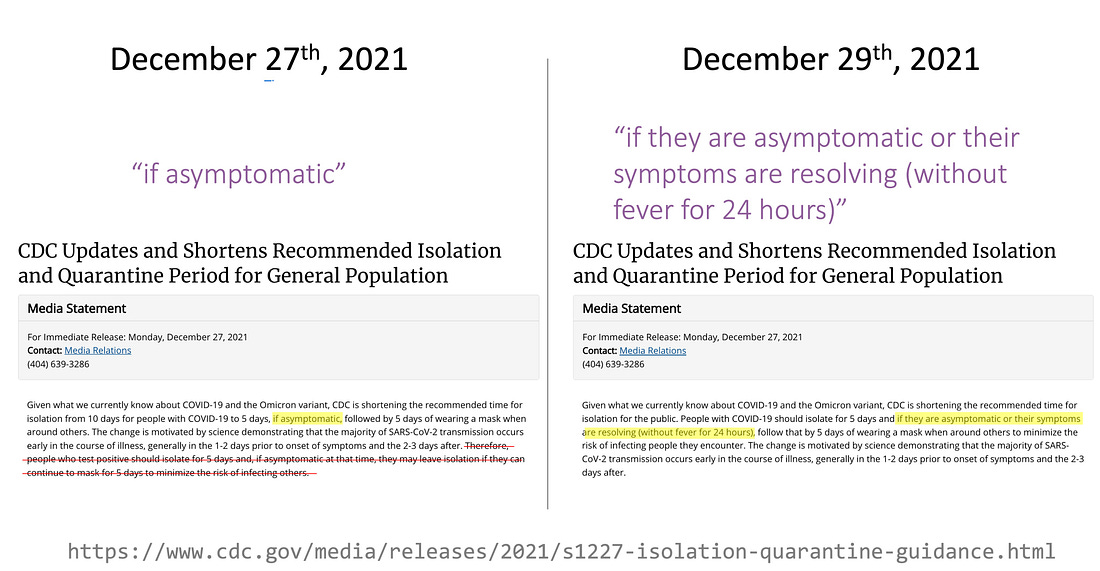
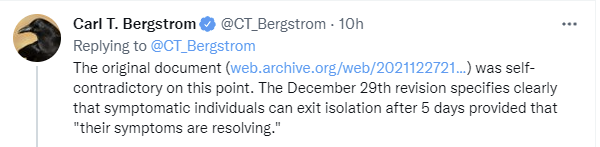
First off, there’s no longer any ambiguity about what happened here, I mean, ’cmon.
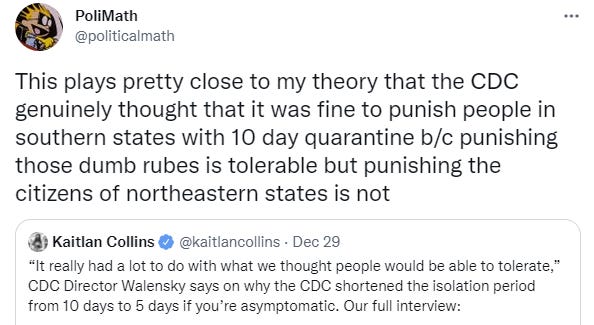
While his hypothesis cannot be confidently dismissed, I am not as cynical in that particular way. I think the CDC simply does not care about your life and how much they mess it up, they care about ‘public health’ as a sacred value. Except they do care if the metaphorical and also literal trains stop running, or what guidelines people would simply ignore, in which case compromises get made. They care, as Walensky admits, about what people ‘will tolerate’ so the whole game doesn’t fall apart.
I believe Fauci here, sometimes authorities do tell the truth, it’s how they keep us on our toes.
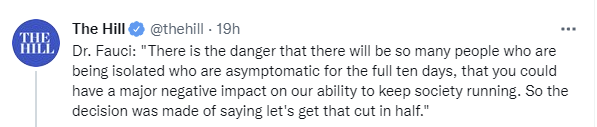
And again, that is exactly what we should do. If society wouldn’t run under your rule, you need a new rule. The rules are made for man, not man for the rules. That shouldn’t require the threat of full breakdown of basic functions of society, but that’s better than actually letting basic functions break down.
And when that happens, you should say that this is what happened, explicitly, exactly like this.
Here’s the top reply.
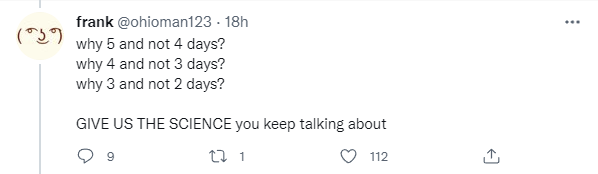
Actual answers, in order of importance, not kidding, here are the Five Good Reasons:
Generation time is down.
Five days is still most of the infectiousness.
The chorus of ‘we must stop this or at least slow it down’ will always give the same answer, so their statements mostly aren’t useful evidence.
Is five days a reasonable rule? How well does it work? Does the math make sense?
I totally agree with Mina that a standard that includes testing would be better, but I don’t see this as a strong response to Walensky here. About 30% of people being infectious on days 6-8 is fully compatible with 85%-90% of transmission happening in the first five days. If we do a quick very wrong approximate calculation and assume everyone is infectious days 2-5, then 30% also infectious on days 6-8, then that’s about 82% of infectiousness in the first five days, so it wouldn’t take much gradual additional decline to get to 85% or even 90%, and we can use whether you’re symptomatic as an additional filter on top of that.
This is the traditional argument between ‘X is true on average’ and ‘X is sometimes false in a particular case’ over which one matters in a given situation.
If we didn’t have rapid tests and could only do PCRs that come back positive for way too long and thus aren’t useful here, would five days look reasonable? Under current circumstances, absolutely, yes. If 10% of London or New York is infected at once and you’ve waited long enough to deal with 90% of your infectiousness already, how much riskier than average are you at that point? Are you making things meaningfully worse by not isolating?
Once you have the option of a rapid test, there’s the chance it might come back positive, so that makes such actions more blameworthy, but it doesn’t make the average outcome worse when you have the opportunity to do better. So yes, we should do better if we can.
The bottom line issue is that it is now an online meme joke that the CDC has no credibility (and before taking this seriously again, here are my favorites from the last day or so, apologies in advance).




And we’re back.
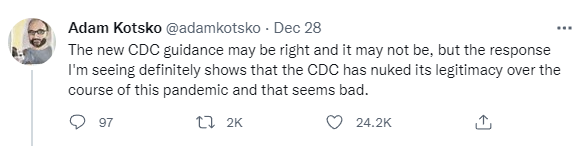
As usual, it’s worth noting that the CDC nuking its credibility is bad to the extent that the CDC is credible, but is good to the extent the CDC is not credible. Better that more people have an accurate view.
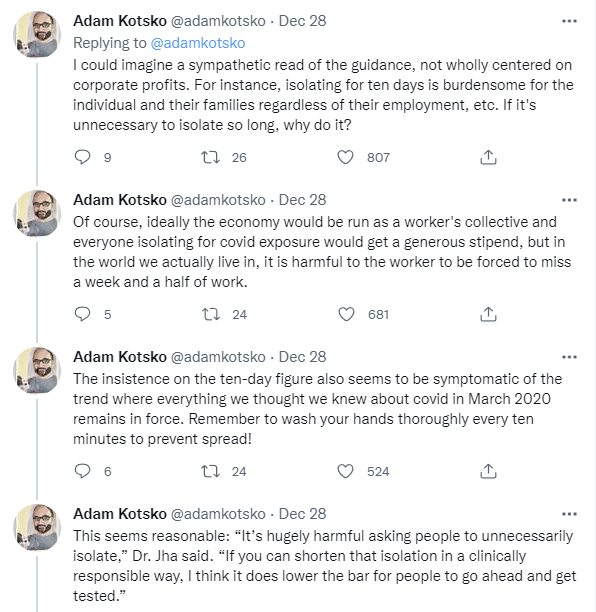

When people say things like ‘I can imagine a read not wholly centered on corporate profits’ even in a thread where every time they look at a particular decision they see good reasons it was made, that does seem like the loss of credibility has perhaps gone too far, CDC Delenda Est notwithstanding.
Also, if people are going to react like this every time you change your guidance to be more lenient (and oh my is it a clear pattern) than the incentives are clear.
Help me debug this, I trained my machine learning system by punishing it every time it admitted its estimates were too high and after the first few revisions it now never lowers its estimates, I have no idea what is wrong and my family is dying.
I continue to be less sympathetic to the stealth edits that have major practical impacts, and a continued refusal (as far as I can see) to explain clearly what’s going on with the whole ‘symptoms are resolving’ clause. If the rule is ‘no fever’ then that’s a clear rule, why not say that?
Are people following the various guidelines? Do they make sense? You tell me.
Testing, Testing, Hopefully
I wrote an entire post last week about the testing situation and how much it was botched. Vanity Fair notices the hole goes even deeper. The medical establishment’s war on testing is ancient, for testing threatens their turf. By which I mean, it wouldn’t be safe, of course. People might act in response to information without proper medical advice. Perish the thought. Can’t be too careful.
So, we ban, then act confused when there’s a shortage.
Remember the thing Biden ‘wished he’d been thinking about back in October?’ Turns out exactly that plan was explicitly proposed.
The plan, in effect, was a blueprint for how to avoid what is happening at this very moment—endless lines of desperate Americans clamoring for tests in order to safeguard holiday gatherings, just as COVID-19 is exploding again. Yesterday, President Biden told David Muir of ABC News, “I wish I had thought about ordering” 500 million at-home tests “two months ago.” But the proposal shared at the meeting in October, disclosed here for the first time, included a “Bold Plan for Impact” and a provision for “Every American Household to Receive Free Rapid Tests for the Holidays/New Year.”
I don’t think Biden is lying here. He does wish he considered it, which means he didn’t consider it, which means that he isn’t thinking about concrete policy proposals. He is not running the show or even thinking about how the show might be run. Staff is in charge.
The administration instead, as we all know, chose to mock the very idea.
On December 2, with omicron threatening an imminent wave of new infections, Biden announced a smattering of smaller-scale plans that included requiring insurance companies to reimburse privately insured patients who buy at-home rapid tests, which sell for as much as $35 for a box of two tests—if you can find them amid widespread shortages. Four days after that, White House press secretary Jen Psaki seemed to deride the very idea of free nationwide home tests. “Should we just send one to every American?” she mused sarcastically from the briefing room podium. “Then what happens if you—if every American has one test? How much does that cost, and then what happens after that?”
Did that many doctors didn’t merely oppose at-home HIV tests on the pretext of patients potentially doing something after learning important life information, they also opposed at-home pregnancy tests for the same reason?
Once Mina began to advocate for rapid home tests, he encountered the same mindset: doctors “trying to guard their domain.” Some doctors had long opposed home testing, even for pregnancy and HIV, arguing that patients who learned on their own about a given condition would not be able to act on the information effectively. Testing, in this view, should be used only by doctors as a diagnostic instrument, not by individuals as a public-health tool for influencing decisions.
A similar view prevailed within the FDA.
Most of you already know this, but it’s worth hammering home how different the testing situation is in Europe than in America:
With roughly 200 different home tests approved in Europe, the price is as low as $1.50 a test, said Schatz. “You go to offices and meetings, you see these tests lying around. It’s a free giveaway, like masks.” Schatz says the prevalence of home tests reflects a different mindset: “I really like the aggressive use of testing and the acceptance of this being a key pandemic tool and embracing the value of information, which tests provide, and accepting some of the weakness.” By contrast, some of the biggest testing companies, from Siemens to Roche, have not had rapid tests authorized by the FDA yet.
Yet even with that level of dedication to supply, Omicron has already overwhelmed demand, presumably because behaviors under virtually-free testing burn through tests at an astonishing rate, because why wouldn’t you do that?
The U.S. is not the only country facing a shortage of rapid tests, as omicron sweeps the globe. This month, the British government ran out of rapid tests that it distributed through an official website. In Spain, pharmacy shelves were empty of rapid tests, after demand rose 500 percent in November. In Canada, after provincial governments vowed to distribute millions of rapid tests at pop-up sites, many citizens seeking them went away empty-handed.
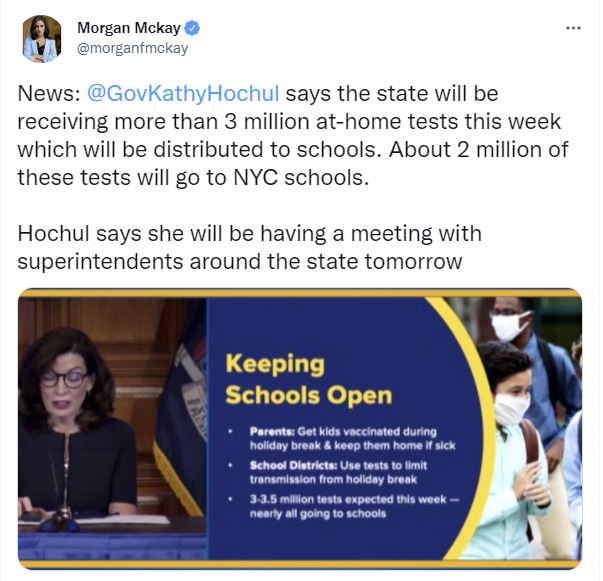
What tests we do get are then going largely to schoolchildren so we can feel better about sending them to school, rather than reserving them to do anything useful. Symbolic use over actual use.
Good news is that we’re now producing tests ‘as fast as we can’ given the restrictions imposed, and the fact that it’s too late to do most of the things that would expand production.
Even better news is that it seems we have approved an additional rapid test from Roche. And then another, from Siemens. Every little bit helps, even when it’s both too little and too late. Go ahead, take your victory lap, I’ll take what I can get.
Testing lines were super long before the holidays, but that could have a lot to do with paranoid relatives demanding extra tests. Whereas this week the kids are off school and don’t require tests, and the gatherings are over, which may explain why I saw one test tent on Sunday night with no waiting line.
Others are paying $300 per test, and also suggesting the correct market solution. More thinking like this, please.
Testing situation is quite bad in the UK (source).
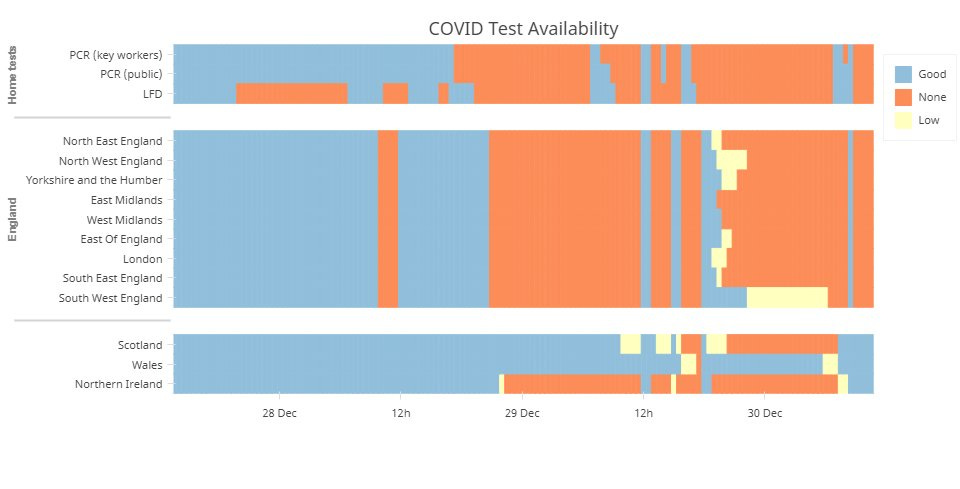
Testing in some places was outright impossible even when urgently needed. While we’re allocating tons of tests to schoolchildren, the hospitals don’t have enough?
Also worth noting that rapid tests do have false negatives especially as used in practice rather than in theory, on top of the thing where they’re testing infectiousness rather than whether you have Covid.
Meanwhile, you heard it here first, the origins of the next supervillain.
Another interesting Christmas anecdote, from the comment section:
Anecdote from the holidays about the difficulty of deciding how to use testing:
Big, difficult-to-arrange extended family gathering (~20 adults) with agreement that everyone would rapid test on the day of. Christmas morning rolls around and a crucial participant tests positive. We give her another rapid test from a different brand. Negative. A third rapid test from the same box as the first. Positive. We scramble and fortunately find a PCR site that can get us same-day service. Negative. Apparently the original box was one of the ~1% of lots that produces a false positive. But we burned through most of our spare rapid tests and most of Christmas Day figuring that out.
Arguably we got unusually unlucky with the false positive, but in the aggregate something like this was pretty likely to happen and it’s difficult to know how to follow up on a positive rapid test.
If someone at our gathering had a positive test, we would have cancelled for sure. This seems like going above and beyond, the person must have been very crucial. I do suppose multiple negative tests from multiple other sources can point towards ‘this box is faulty’ but it seems tough to be confident about that. What I probably would have done is give someone else who tested negative a test from that same box you are worried about?
Long Covid

I’m surprised that 61.9% of positives had already been caught by PCR.
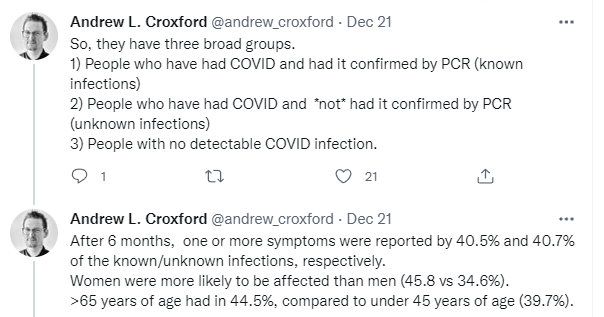

Finally, a control group, and it looks like it controlled for quite a bit.
Assuming this is being reported correctly, it’s saying that if you have an unknown infection, you don’t get meaningful Long Covid.
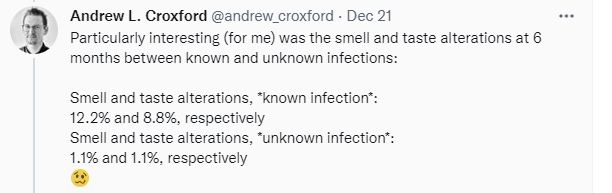
This at least rules out the hypothesis that Long Covid is a threat in asymptomatic cases. If you don’t realize you had Covid, your rate of reporting symptoms doesn’t rise, at least not a substantial amount.
We could in theory give the benefit of the doubt that everyone with symptoms got a PCR test, but I’m still awfully suspicious of zero effect, especially when other claims sometimes involved not differentiating much based on severity of the infection.
To the extent that Long Covid is a non-placebo Actual Thing, this seems to strongly suggest that it will indeed scale with the severity of infection, so vaccinations and booster shots will help a lot, and if you’re at low risk for Short Covid (as it were), you’re also therefore not at such high risk for Long Covid either. The idea that children were getting permanently crippled by otherwise harmless infections all over the place doesn’t match this data at all. Long Covid, and the rise in morbidity in the year after Covid infection, are likely the result of Covid infections that get bad and do a bunch of damage.
That also implies that Paxlovid and other early treatments will improve Long Covid outlooks.
Think of the Children
If you play to win The Game, and for one shining moment you do, then your students are going to get excited, and proper pandemic strategy is going to get weird.
This for once is not me making fun of Michigan University and its football program. Not only did they beat the dastardly Ohio State and make the playoffs, of course they’re underdogs who might be overmatched but I still think that over all possible worlds +7.5 against Georgia is good value, and they’re asking the right questions. So this, but unironically.
No, really, this is exactly how epidemiology works. You’d prefer people not congregate in one place and throw parties together. If they’re going to do that regardless, it’s no longer a consideration in deciding whether to do something that would cause that, like bringing students back to campus, or even scheduling classes. It’s about physical actions that cause physical risks, and doing the math.
And of course, no such situation would be complete without blaming the CDC for the one time it tried to be compatible with life.
Again, that is exactly right. The CDC guidance would otherwise make the living of life impossible. By making it possible, they opened the door to life being lived. Oh no.
They are also mandating booster shots be completed by February 4, at which point the booster won’t accomplish much, but mostly that’s a shrug.
A Note on “Remote Learning”
Marginal Revolution linked back to this 2012 post on Why Online Education Works. It is an excellent post, treating online education (as opposed to online school) as an opportunity to improve rather than a burden of mimicry.
I see three principle advantages to online education, 1) leverage, especially of the best teachers; 2) time savings; 3) individualized teaching and new technologies.
That seems exactly right. When you are doing online education you get many huge benefits. Everyone can:
Get the best teachers.
Take the best classes.
Get the best version, with extra preparation time, designed for remote learning.
Take the classes they care about.
Take classes on the schedule that works for them.
Go at their own pace, pause, watch again, review.
Use the internet and other new technologies as resources.
Have zero marginal cost.
Ask questions and get answers.
Put the focus on learning rather than time spent or credentialism.
Now look at what we did over the pandemic with ‘remote learning’ and notice we got at most two and arguably none of these ten advantages.
Some implementations gave students (9) the ability to ask and answer questions, or to some extent (7) use the internet, but that’s about it, and not consistently or at full power.
They definitely didn’t get any of the (1) best teachers, (2) best classes, (3) best or properly customized version, (4) that they care about (5) on a schedule that worked for them (6) at their own pace (8) at zero marginal cost (10) with a focus on learning rather than time spent or credentialism.
Instead, we did our best to duplicate the physical classroom with all its problems not only intact but amplified by having to implement them via screens.
Students got their old teachers, who had signed up for a very different experience and many of whom (very understandably) hated their new jobs, teaching the same classes they always had, with little time to prepare for this entirely different world. Laser focus was often on whether a student was physically at a keyboard, or even looking directly into a camera, because otherwise they wouldn’t get credit for time served. That meant periodic checks to see who was ‘present’ and ‘paying attention’ which rules out any attempt to actually learn via going faster or slower, or focusing where one is confused or curious. All the innovations we’ve had over decades in online learning were ignored in favor of a zoom call, and all in the service of not ‘missing school.’
Is it any wonder kids hated it, didn’t learn and became depressed?
We have tons of great educational tools to teach kids things on tablets and computers, including educational games and Khan Academy and lots of other things designed for the medium, or by reading books (yes, books still exist) or playing with physical objects, or listening to the radio or audio books.
In Other News
Gain of function research finally has someone willing to stand up and defend it.
Exactly right. At best, this piece what we like to call ‘complete and utter bullshit.’ The argument is that technically ‘gain-of-function’ includes any attempt to do almost anything, so of course ‘gain-of-function’ as in ‘let’s make this virus more dangerous to see what would happen, no it won’t leak what are you talking about that definitely never happens, things don’t escape from labs’ must be fine.
No, seriously, this the line chosen here (and this is Stat News, which is normally excellent, so I can’ consider this a strawman):
Johnson & Johnson’s Covid-19 vaccine is a gain-of-function approach. It uses a type of virus called an adenovirus to deliver a portion of the SARS-CoV-2 genetic material to the body’s cells, where it stimulates an immune response that protects people when they become infected by SARS-CoV-2. Adenovirus does not naturally produce this genetic material: It was engineered to do so through gain-of-function research. This general approach is not unique to the SARS-CoV-2 vaccine; vaccine production has long been supported by similar gain-of-function approaches.
I’ve got a suggestion. We get together and work out a definition that allows ‘gain-of-function’ when the function is engineered to be part of a treatment or delivery system meant to be put into humans we’re looking to help, and differentiate it from ‘gain-of-function’ when it involves the virus gaining functionality in terms of its ability to infect, sicken and kill us, no matter how many times you say it would help you ‘see what happens.’ Or alternatively, you notice the definition in the existing bill proposed already does that. Capiche?
If this is what a defense looks like, there is no defense.
Some have even called for an end to gain-of-function studies altogether without recognition that it is a widely accepted research technique employed by scientists around the globe.
Doing that would be short-sighted.
With the push to negotiate and pass the U.S. Innovation and Competition Act, which includes language that would have harmful ramifications on viral gain-of-function research, it is imperative that Congress modifies the act before the landscape of research is altered for decades to come.
Oh, we’re fully aware. We recognize. If it wasn’t a research technique scientists were employing, we wouldn’t need to ban it. That’s exactly the problem.
So this is excellent news, that there is indeed an attempt to do at least something about Gain of Function research. I’d love to be at ‘and then they fight you’ on this one.
New York City cuts quarantine period to five days for ‘essential workers’ including not only health care workers, but grocery store workers, teachers and nursing home workers.
“Phew, so if you work in one of those Targets that has a frozen food and granola bar section – 5 days,” New York City Councilman Joe Borelli wrote on Twitter. “Work at the other ones – 10 days, it’s just not safe. Together we can stop the spread. #science”
…
“We need you again, we need you to be able to go to work,” Governor Hochul said.
Full official guidance here. As the opposition points out, five days either is safe or isn’t, and nursing home workers are the worst possible place to bring people back early, for obvious reasons. The ‘official’ positive rate is 0.3% of the population per day in NYC, and the actual rate much higher. It would be more dangerous to have health care workers wait ten days than to wait five days. Do we draw the same line at grocery stores, or accept longer lines at grocery stores?
WHO Delenda Est, they really are doing their best to kill you. If it was intentional, how would they act differently?
More of the same WHO talk later on.
Note that a booster is actually more efficient at protecting against Omicron than the first two vaccine shots, so this is malicious on even more levels than it was before.
Finally, if it’s this easy and all he really wants is a little respect, sounds good to me, let’s do as this man likes to do, and make a deal.
Trump is also on message regarding those vaccines, without insulting the people he’s addressing. It’s not working, exactly, but I’m sure it’s doing some amount of work, and if he’d wanted to Trump could have caused quite a bit of trouble. Getting and staying on message can’t be easy here, but it’s both smart and the right thing to do.
Press release announcing Vitamin D makes symptoms go away faster in Phase II trial. Technically the trial is for a delivery method of Vitamin D called Rayaldee, because adding a time-release system allows for a patent and some of those sweet, sweet monopoly profits off of captive insurance companies, which is how you bankroll approval from the FDA and also how you profit from something like Vitamin D. Not the best system, but a good reminder that this is one of the lowest hanging fruits, and the only active supplement I currently take.
A claim that Paxlovid will be hard to scale because of scarce ingredients, no idea extent to which it is true.
I’ve come around to the position that Molnupiravir should not have been approved because of the danger that it will create new variants. It’s a private good at the cost of a public risk, and I don’t believe we can trust people to take the drug as directed to ensure nothing bad happens. I don’t know the magnitude of the risk, but the precautionary principle attaches here, we should not have done this and I should have realized it sooner without needing to see so many others making the point.
And no, seriously, never do this.
Also don’t respond to people’s taking positions you disagree with by attempting to shut down debate, which seems to have been our government’s reaction to proposals to reopen things before Very Serious People thought we were ready to do that.
Masks better than N95s are one of the best ways to get real protection and actually have a shot at avoiding Omicron. Alas, people often don’t let you use them, such as this account where someone who was immunocompromised wasn’t allowed to use one on a flight, and thinks that’s how they got Covid-19.
Helen Branswell’s ten lessons from the pandemic.
Current Paxlovid prescription requirements in New York. Seems like we’ve chosen to skip the impossible choice by simply not making deliberate decisions at all and seeing what happens. If our logistics are incompetent enough it might even work.
Thread calling for a return to normal.
Not Covid
More details on the history of attempts to stop at-home pregnancy tests.
SMBC asks what counts as science. Or is it what counts as Science(tm)? That is the question, after all. I do think it’s true that (almost) every human who ever existed for long did at least some science, the same way they also all did math. I also think it’s true that most ‘looking at thing’ does not count as Doing Science To It, the same way that most practice is not deliberate practice and mostly doesn’t count, but that has nothing to do with following standard protocols.
A thread from Patrick McKenzie about an employee who quit, and some good related advice about one’s relationship to one’s job. Such epic fully avoidable failure. I’ve always been one to do what needs to be done when it needs to be done, but also true rest time must be scheduled regularly and guarded absolutely or it doesn’t exist.
Wow. Jordan Peterson joins the ranks with Bret Weinstein of people who had their brains and imaginations scrambled during this culture war battle. I don’t want to be too harsh about it, we’ve all been there at some point, but it’s really really hard to watch.
I was surprised too. Moreover, he is vaccinated, so I don’t really understand that response
Someone commented on the same post at Zvi’s blog claiming that there is a specific history of related ‘moves’ (by the Canadian government) that provides a context for a more charitable reading of Peterson.
I think the tweet about the NHS app(s) is slightly misleading. I’m pretty confident those screenshots relate to two separate apps: one is a general health services app which can also be used to generate a certificate of vaccination (as the app has access to health records). The second screenshot relates to a covid-specific app which enables “check-ins” at venues for contact-tracing purposes, and the statement there seems to be declaring that the local information listing venues visited could—in theory—be used to get demographic information. One is called the “NHS App” and the other is called the “NHS Covid 19 App” so it’s an understandable confusion.
Yep, I’m removing it to be safe.
Nit: Does the linked tweet say the person was in contact with an immunocompromised person, rather than immunocompromised himself?
“Half the people who aren’t vaccinated have sufficiently strong priors against doing anything new that they’re having none of it, it all sounds super suspicious to them, and you’re not going to tell them different. The alternative hypothesis, which I find less plausible, is that the political divide carries over to everything else automatically at this point, which is functionally the same but has some different implications.”
Could a significant number of people refusing both vaccines and Paxlovid be biased against Pfizer?
There’s at least some possibility that it’s less of a Pfizer bias than it is an “unnecessary medical intervention” bias (my family of origin made sure we all got our 1980s-recommended vaccines, but they also said “taking Tylenol for a headache doesn’t solve the underlying problem, drink a glass of water instead”). You may believe that Paxlovid could be helpful in some situations but you’d rather not take it unless you absolutely have to.
That said, we’ve also been exposed to two years of “this will work!” followed by does not work, does not work as promised, or reliable sources come to different conclusions about efficacy, and at this point it really doesn’t matter if you think the vaccines are full of nanobots or if you think they lead to an increased risk of myocarditis because the actual fact on the ground is that the vaccines may reduce [spread, severity] but they do not work in the way that we were initially told they would work.
Therefore, the claim that Paxlovid “will work” is automatically suspect, whether or not it should be.
[If] that many doctors didn’t merely oppose at-home HIV tests on the pretext of patients potentially doing something after learning important life information, [did] they also oppose at-home pregnancy tests for the same reason?
EDIT: fixed a typo relative to tense change:
opposed → oppose, which this texteditor auto-in-corrected.
(I still think the question is better if ‘for the same reason’ is also omitted. Other possibilities may be hypothesized.)
Apparently yes!
It wasn’t a question. It was a suggested change in that question, the text of the Original Post, as it were, to make it more readable.
(I also edited my comment after noticing another ‘typo’ in the section you quoted.)
My bad!
It was not at all clear tho that you were offering corrections.
Having spent the past week (technically, the past month) being the House Hero in all matters related to holiday prep, well — I mean, I can’t say this is the case in the commenter’s situation, but in my household the amount of holiday planning knowledge (where the special dishes were located, where the special recipes were located, which family members have which dietary restrictions and preferences, etc.) that I was carrying, organizing, and delegating was in fact crucial.
This is definitely an important question but it doesn’t seem to me as so wide open a question. I think the prior (i.e., established POV of “Science”) is just your model, and I think the evidence is consistent with that. The natures of the humoral and cell-mediated immune systems would seem to suggest that if you have few or low-capability antibodies/cell instructions, you’d be more likely to get sick, and that at a critical mass, you’re functionally immune because anything that enters will get dealt with (e.g., think border patrol). This would look like a sigmoid curve relating neutralization titers to vaccine efficacy.
If you take a snapshot of neutralizing titers on average induced by a vaccine vs. efficacy, then you could naturally wonder if this is just because of a heterogeneous immune response in the population (and/or sampling over time, e.g., although the average time since dose may be X, some samples may have been taken at X+30 days and therefore have lower levels from natural clearance over time) or if it’s simply probabilistic. Once you see titers over time and/or for multiple vaccines, or at the individual level for multiple people/samples, you can test whether that variability matters, and you can find that indeed immune responses are heterogeneous (not just binary though), resulting in functional immunity around a threshold titer level and probabilistic immunity below that (and as commonly assessed, those categorized with serological non-responsiveness below a lower threshold). Not surprisingly, the titer vs. efficacy relationship is sigmoid.
In fact, neutralization titers represent the amount you can dilute a sample while still preventing infection in 50% of inoculations (the more you can water it down while to get it down to 50% “efficacy,” the more antibodies there must be), so there is a probabilistic component even at that point (or at least error terms to our model), but certainly “the more [antibodies], the merrier [the human],” and at some point you have so many antibodies floating around (or your body can whip them up on a dime, for other diseases) that you’re functionally immune.
The case isn’t closed, but your model is the prior, the prior is your model. Woo!
Does anybody know what is the best mask that they’ll allow you to wear on an airplane? Has anyone worn a P100 with the exhale valve covered, or do they not allow that?
i have worn this on an airplane with a surgical mask over the exhale valve
https://www.amazon.com/GVS-SPR457-Elipse-Respirator-Medium/dp/B013SIIBFQ/ref=sxts_rp_s1_0?cv_ct_cx=gvs+elipse+p100&gclid=CjwKCAiAzrWOBhBjEiwAq85QZyLzBYwxwOZcFGAMZbn4S6OVwxcQXnl1L6L9xWu1dQgzAFdKK8oxOhoCqo0QAvD_BwE&hvadid=409918312011&hvdev=c&hvlocphy=9014238&hvnetw=g&hvqmt=e&hvrand=6118992613772945421&hvtargid=kwd-267611734495&hydadcr=20509_11115072&keywords=gvs+elipse+p100&pd_rd_i=B013SIIBFQ&pd_rd_r=03b1c070-7191-4557-b0bb-79b3930e0ac8&pd_rd_w=JYxDi&pd_rd_wg=uF7dV&pf_rd_p=53ef7f8b-c1cb-4ebe-8d67-39f3ca0ebaf7&pf_rd_r=PE758N16XDW0FMZ1MZXD&psc=1&qid=1640904683&sr=1-1-5e1b2986-06e6-4004-a85e-73bfa3ee44fe
Me too, except my P100 was wearing a cloth mask rather than a surgical mask.
And would a doctor’s note make any difference towards them allowing you to wear something like a versaflo or other PAPR?