I have a lot of open tabs from today’s incoming information. They are all about Bing, and its new AI-enabled chat. It is rather unhinged and engaging in a wide variety of hostile and manipulative behaviors. One hopes this will lead to some realizations about what things can do or some hesitation about hooking them up to the internet. Alas, I am not holding my breath on that. I half-joked that I’d have to switch to weekly AI posts, and all the replies took it fully seriously and were highly positive. Interesting times will continue, I suppose.
I had a bit in here about Scott Alexander’s noble attempt to stand up for thinking for one’s self, but then he did another post in which he was largely against that, so I’m taking that out for now and will work on it more, likely post it on its own at some point.
Covid times? Boring. Which is great.
Executive Summary
Situation continues to slowly improve.
Eric Topol even more wrong than usual.
All the news is now about AI and Bing instead. It’s going great.1
Let’s run the numbers.
The Numbers
Predictions
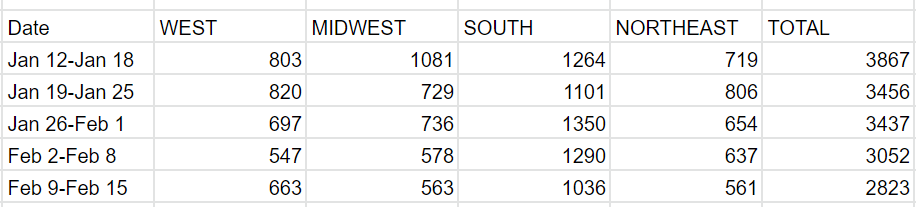
Predictions from Last Week: 220k cases (-7%) and 2,750 deaths (-10%)
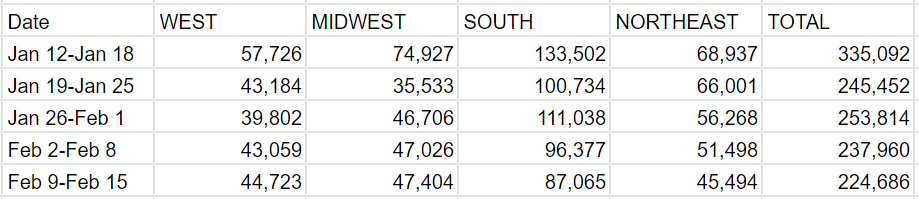
Results: 225k cases (-5%) and 2,823 deaths (-8%).
Predictions for Next Week: 210k cases (-6%) and 2,625 deaths (-7%).
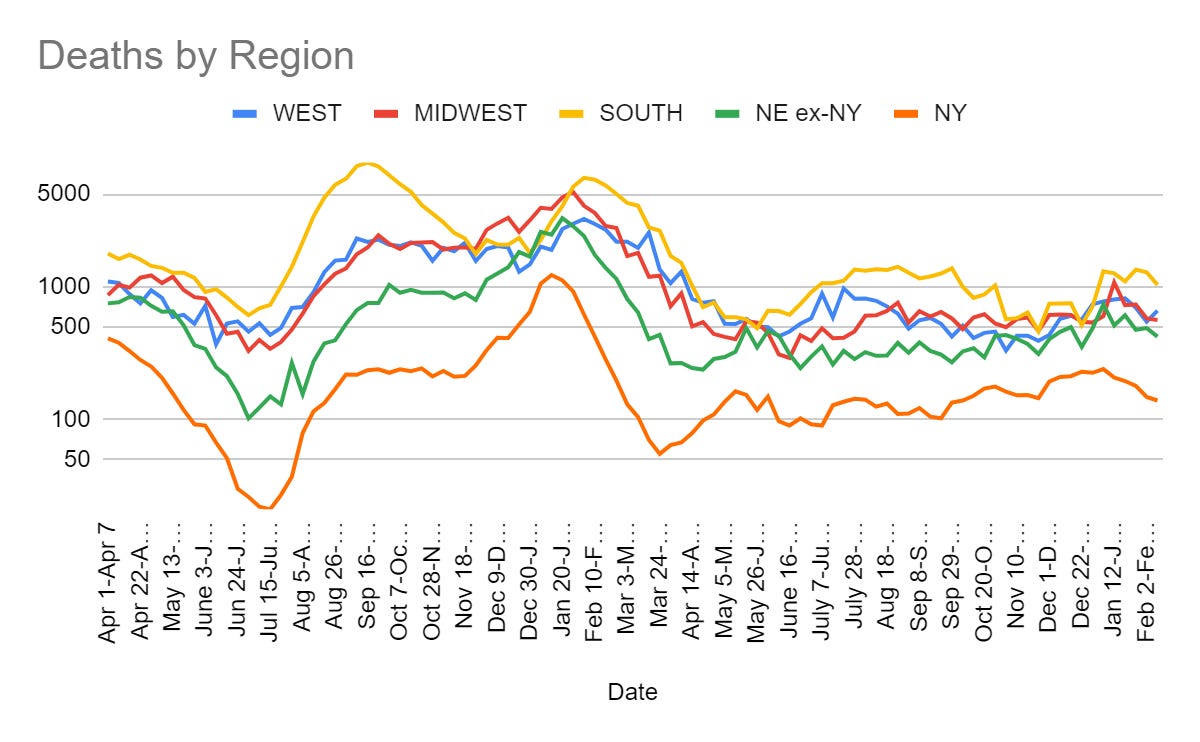
I see no reason not to expect continued slow but steady declines.
Deaths
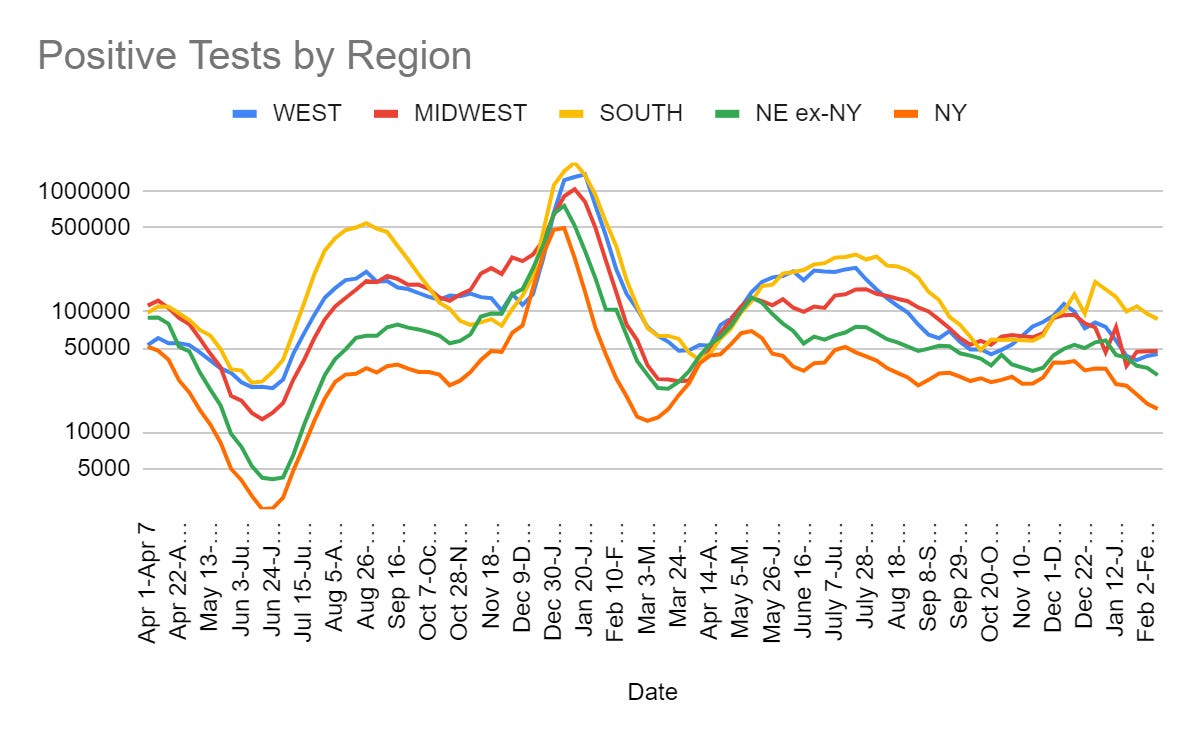
Cases
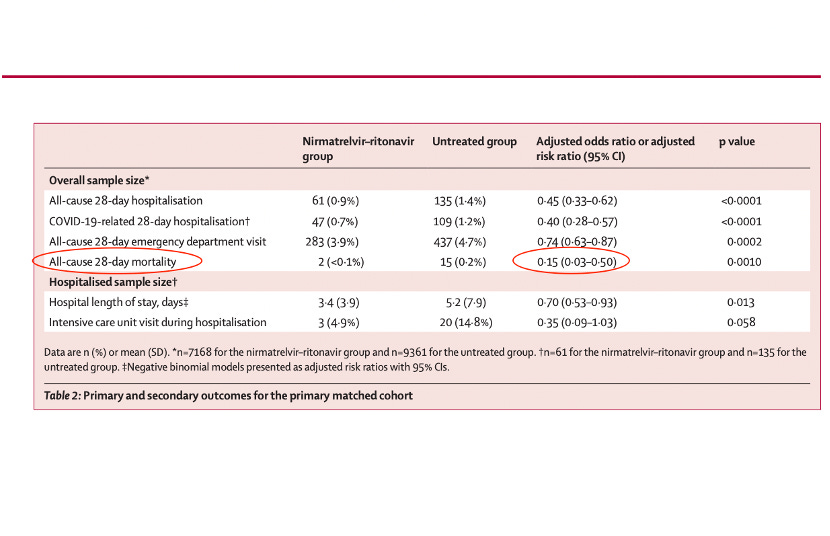
Eric Topol and The Obvious Nonsense Paxlovid Study
In a better world, no one would ever listen to a single word Eric Topol had to say. His record of reacting to scientific research is not great. He was also taken in by Theranos. And then there was the time he was instrumental in sabotaging approval of the Covid vaccines so that it would happen after the November election. Oh. That.
Alas, the world is small and contains few people, and somehow Topol continues to be one of them – he is often the source quoted for some new development, and people share his opinions.
Which, as noted, are often not so smart.
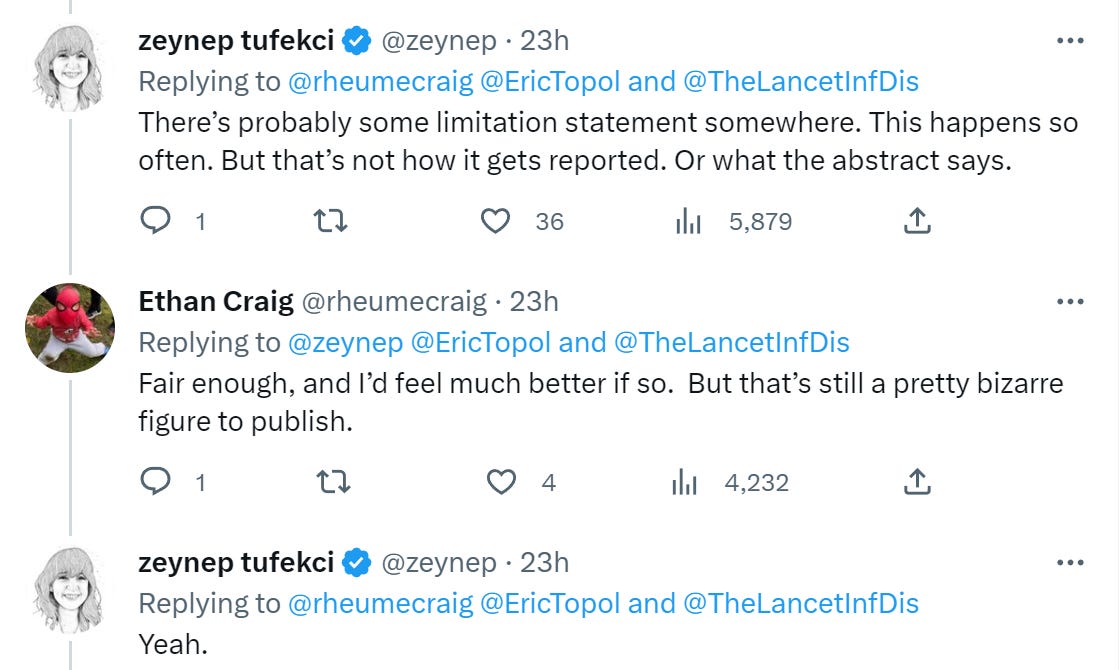
I continue to believe Paxlovid is great and we should be using it more often. This study did not update my belief on that front. It did update me on what we should expect from ‘peer review.’ I mean, wow.
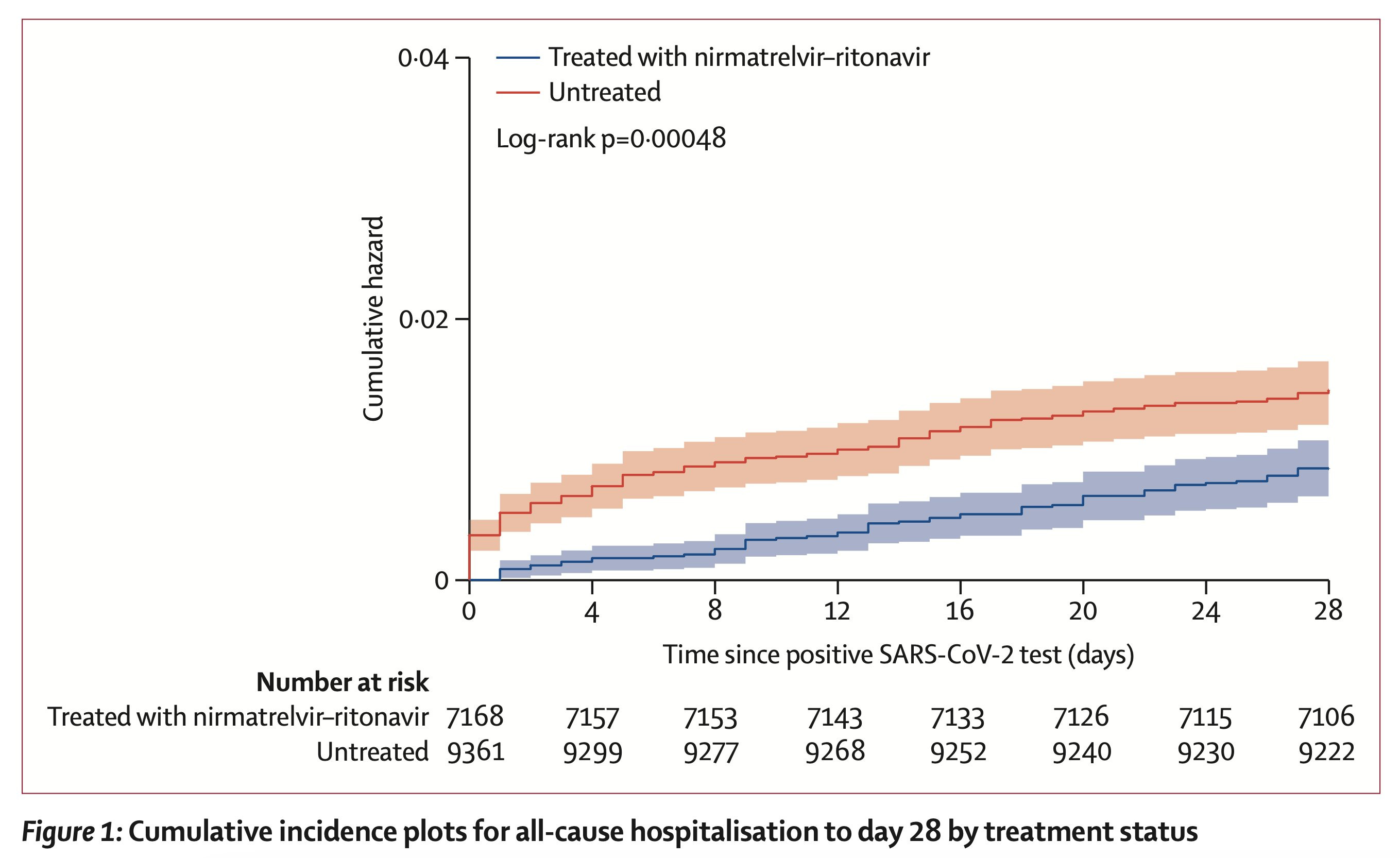
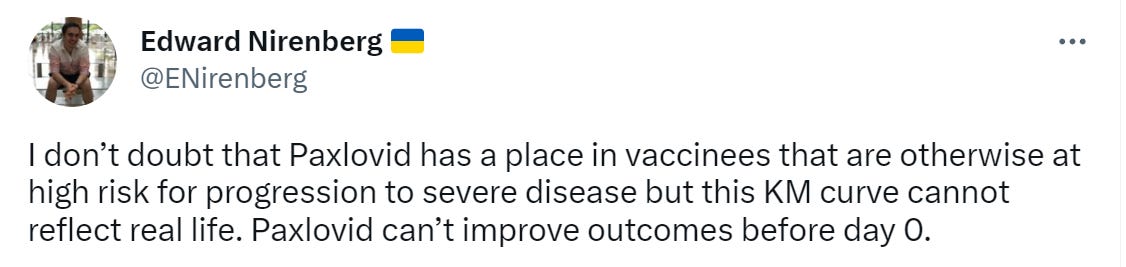
Yes, the treated vs. untreated distinction mostly starts on day zero. Magic. They administer the drug by default on day one.

Explanation for how this happened:
As described in the prespecified statistical analysis plan (appendix 2 pp 3–4), we included all patients diagnosed with SARS-CoV-2 infection identified using electronic health record-based SARS-CoV-2 positive test date (either PCR or antigen test) or nirmatrelvir–ritonavir medication order date if a SARS-CoV-2 test result was unavailable.
…
Notably, most patients treated with nirmatrelvir–ritonavir did not have a SARS-CoV-2 positive test date in the health system electronic health records. Because a prescription of nirmatrelvir–ritonavir requires a positive SARS-CoV-2 test, we assumed that testing occurred at home or at a location outside the health system for these patients. As many patients received antiviral treatment the same or next day after a positive SARS-CoV-2 test, for analytic purposes we used a SARS-CoV-2 positivity test date (the index date) of one day before the recorded nirmatrelvir–ritonavir order date for the primary analysis.
…
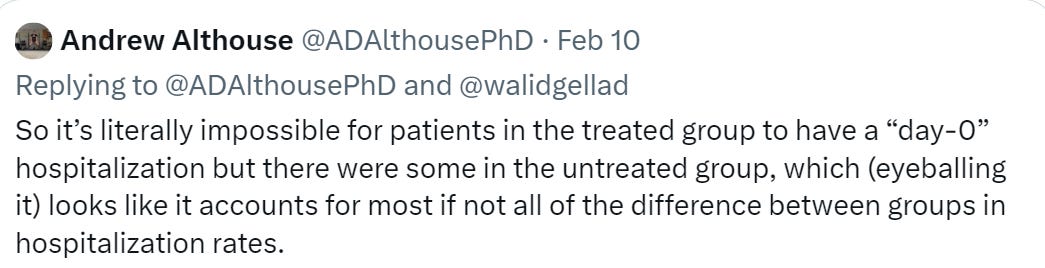
Hospitalisation was defined as any inpatient or observation encounter documented in the electronic health record. We selected the first hospitalisation that occurred the same day, or any day after, a SARS-CoV-2 positive test for untreated patients, or after the order date for nirmatrelvir–ritonavir for treated patients.
Oh. Yeah. That’s… not how any of this works.
I was going to say let’s read the paper, but after looking at the sources above it does not seem necessary to belabor the point.
In Other Covid News
John Hopkins Covid Tracker shuts down.
Another call for ‘deeper understanding of the pathophysiology of Long Covid.’
Projection of a default of ~100k Covid deaths per year in America going forward, potentially more than all other infectious disease combined, and a call to increase rates of up-to-date vaccination to fight this. I see ‘make treatments available’ as far more promising. If we cared, we could properly use Paxlovid and Interferon. We don’t do that.
Remember
New York ended mask requirements at health care facilities on February 12.
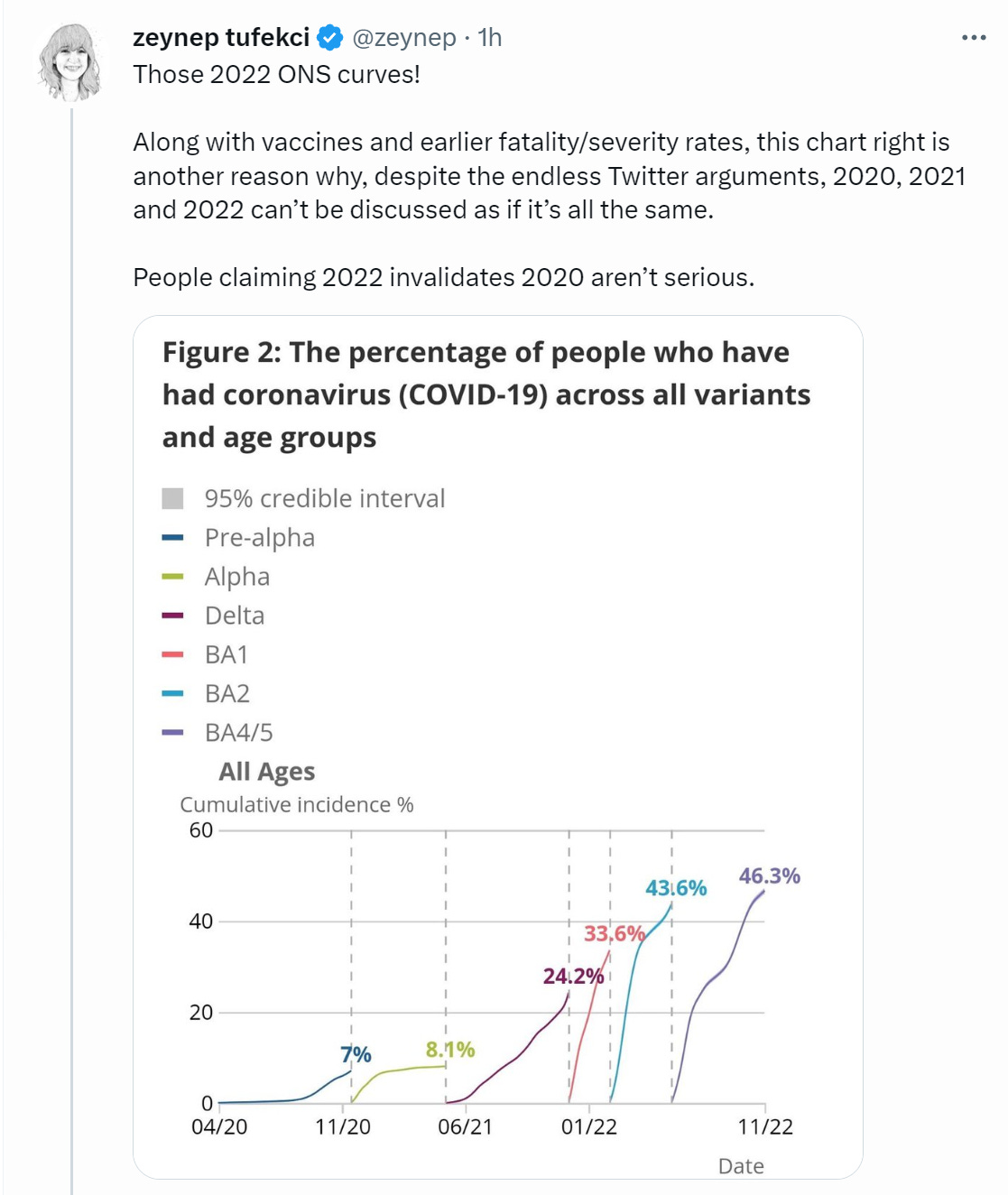
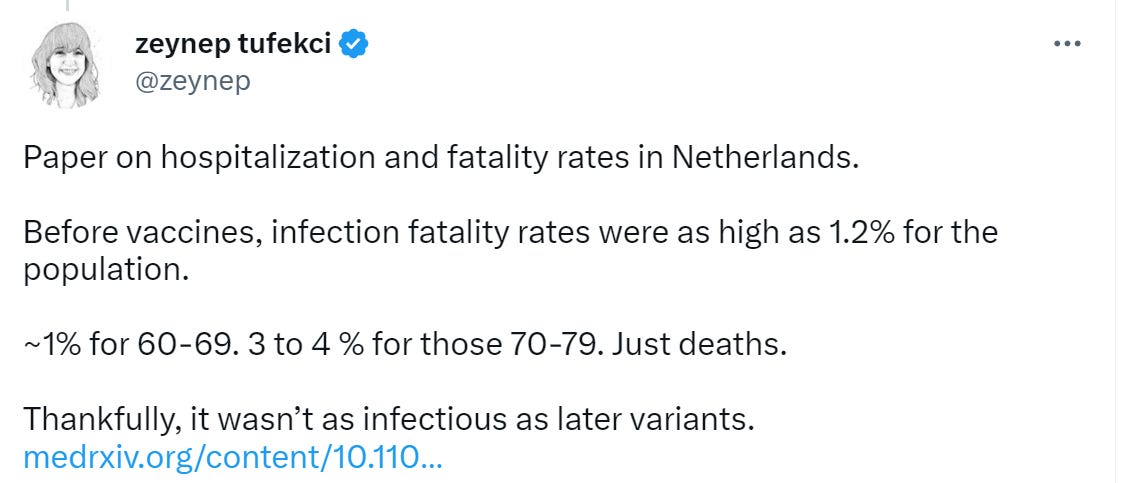
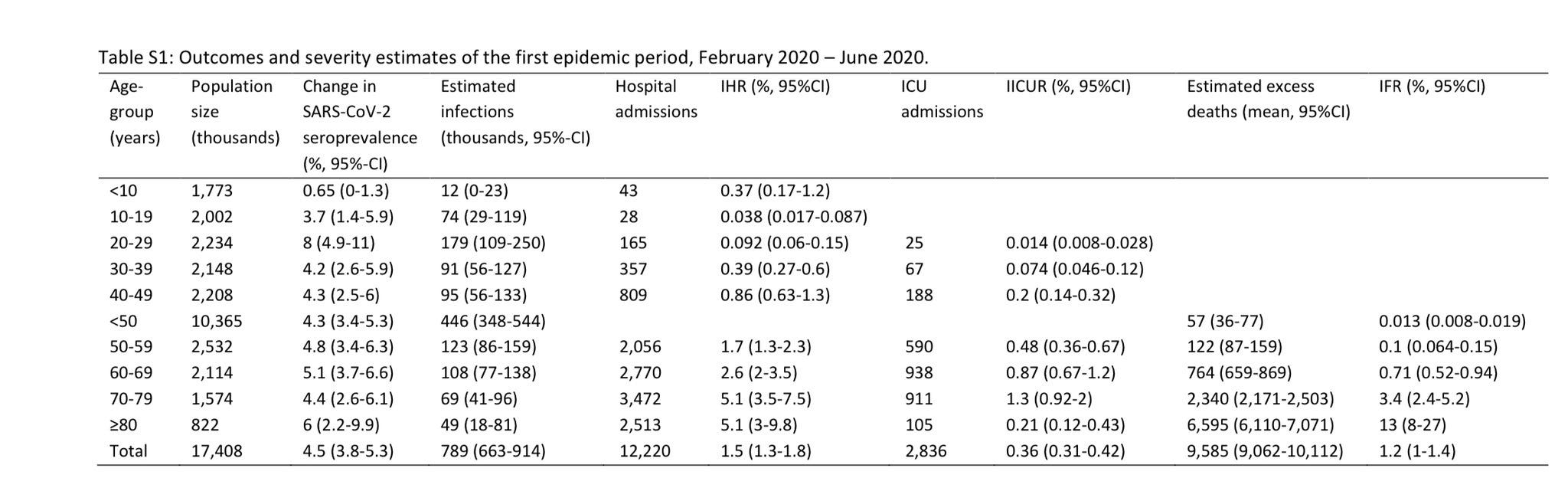
Some ONS curves and old hospitalization data (link to Netherlands data). The risk from a Covid case in 2020 versus the risk from a Covid case in 2022 was night and day.
Heart attack rates were 30% higher than predicted during first two years of the pandemic. Highest relative rise was in the 25-44 year old category, so the speculation is of course that it is their fault due to lack of the prescribed social distancing, masking and vaccinations. Also there was another rise after Omicron. I treat this as a pure ‘yes Covid can cause heart attacks, and this is effectively Covid deaths being counted as heart attack deaths, and it means we are modestly undercounting Covid deaths in this way.’
WHO abandons plans for investigation of Covid origins.

They are who we thought they were. Will we let them off the hook?
Other Medical and Research News
Broad set of Republican politicians across nearly two dozen states file court briefing to ask FDA to withdraw approval for mifepristone, also known as medical abortion.
Medicare setting up a demo to pay less for drugs under accelerated approval, ‘as a way of prodding companies to finish up trials.’ If this encourages more accelerated approvals getting issued, that seems good?
CBD industry begs for FDA regulation, FDA says no, Congress has to do that, otherwise their ‘regulation’ will continue to be the word ‘no.’ Those asking for FDA regulation here seem not to understand the rules of things subject to FDA regulation, especially ones considered inherently suspicious given their origins.
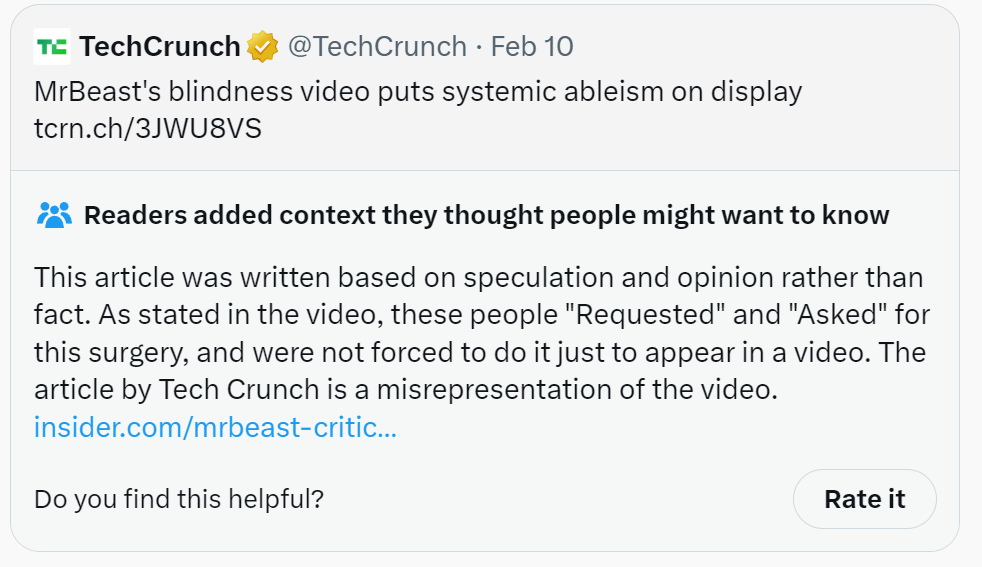
On the MrBeast curing blindness front: TechCrunch, a rather large publication, jumped on the ‘making blind people able to see is bad, actually’ bandwagon, displaying standard levels of rigor. I continue to mention it because it seems important to recognize the phenomenon for what it is, and this is an unusually clean and safe-to-discuss example of a common practice.
This quote is great.
It’s so crazy. I would expect exactly that to happen. I’d even expect someone else to pay the bill for it. And I’d consider it a good thing.
Is this effective altruism? The video has 103 million views, so I’m going to guess that at least for him, given the revenue he got back, this was highly effective altruism. He even also does some of the Giving Directly thing with bonus cash payments, selected in a way that clearly avoids incentive warping.
Also, the intervention? It’s a ten minute surgery that cures some forms of blindness. The typical QALY adjustment for this change looks like it is at least 0.2 or so per year. The surgery looks like it costs thousands to tens of thousands of dollars.
Certainly it more than passes the thresholds for ‘things government should pay for in health care’ and ‘worthwhile use of the physical resources required.’
Is it the best use of funds in its broader cause area, or can we do better? That depends on how much you believe in the effectiveness of scaling alternative interventions.
In case you didn’t know (and I didn’t) womb transplants are totally a thing now, with delivery via C-section. Whole issue is framed purely in terms of the transgender. Womb transplants are good because that is a ‘right’ that cis women have, and now transgender women can do it. Or they can have ‘enhanced gender alignment’ in an invisible and dangerous way. Or a handful of transplants could be used as another reason to attack the words ‘mother’ and ‘father.’ I am happy that we are making progress in such areas, especially as it gives me more hopes for potential future artificial wombs, but it does seem like at least in its current state it is a risky and expensive option compared to surrogacy or adoption.
Another point on Americans getting larger.

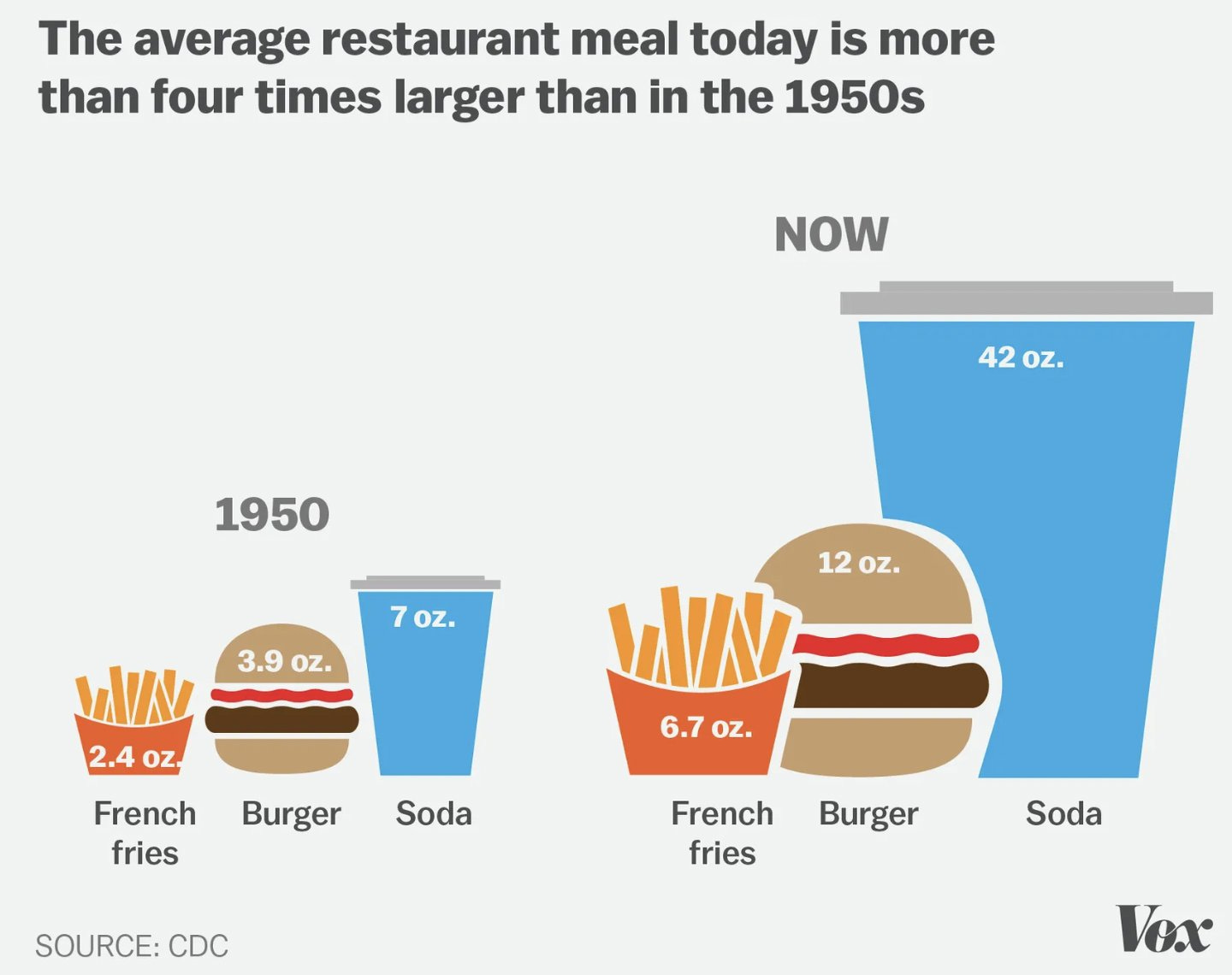
These supersize portions are reflected in our daily calorie intake. The average American’s total caloric intake grew from 2,109 calories in 1970 to 2,568 calories in 2010. As Pew Research put it, that’s “the equivalent of an extra steak sandwich every day.”
Where can I find a steak sandwich with only 459 calories? Must be the 1950 version.
Still, it’s quite a lot of extra calories. My lord, that soda, what the hell everyone. At equilibrium, that more than accounts for all the extra weight gain when I run basic calculations.
None of this has to be a mystery or be complicated. You do not need to buy the full calories in, calories out calculation to say that caloric intake going up is the story here. You can then say that there is a different story about why we all eat so much that is more complicated. The core story could still be summarized as ‘bigger portions of more calorically dense food, everywhere, as the default.’
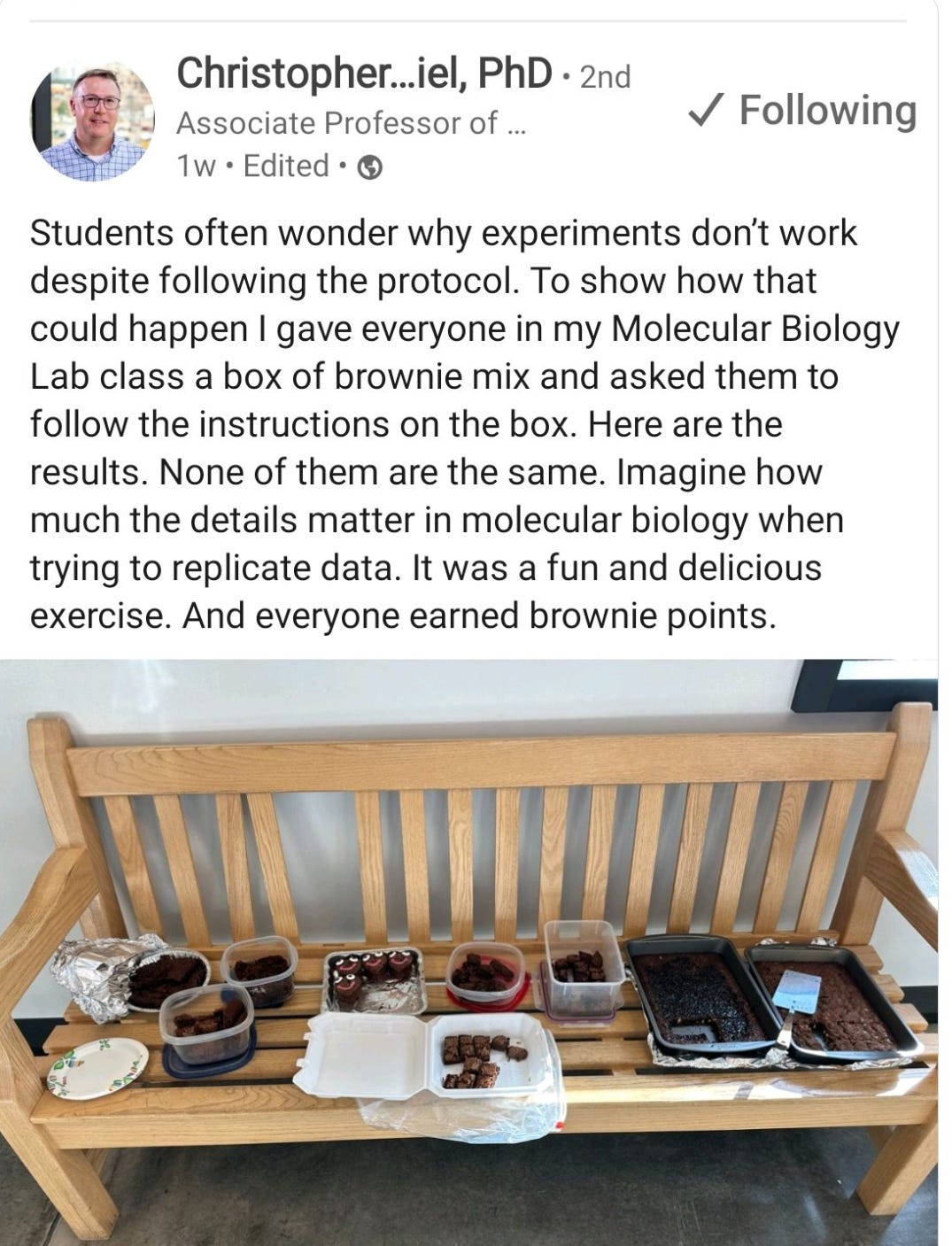
In other relevant and delicious but fattening science observation this week:
By which I mean, we are definitely all going to die, but now it is at least somewhat clearer that we are all going to die, so maybe some people will try to make that not happen.
Yeah, portions are way too big now. I’m 6 feet, 4 inches tall. Having two meals per day is quite enough for me, I only order one thing when I go to restaurants and I’m always too full to eat dessert. If I was a normal height and tried eating three meals per day, I would definitely be too fat.
(To be clear, I’m in the US. It’s extreme portion sizes get commentary from visiting europeans)
Where’s the AI news? Maybe in fact we are “all going to die” from rampant superintelligence, but when?
How much of the flood of AI papers and incremental advances in actually significant?