I’m going back to New York City, baby! Tomorrow’s the big day.
Oh, yeah, the pandemic. That’s still a thing, and one still has to deal with the various ways people are dealing with it. Cases continue to rise slightly, likely due to increased testing, and we certainly aren’t seeing a big improvement on the horizon.
The big Covid development this week was about Long Covid, as we got multiple analysis posts on the subject and some extra data as well. My conclusions on magnitude have not changed much, and I continue to believe that Long Covid is a thing worth some effort to avoid, but it is not as severe or common a thing as some reports would suggest, and that it is not a big enough issue that one should make big changes in life to avoid it, when you compare it to the effects of long-term Covid prevention. This is one of those cases where you are encouraged to run your own analysis, draw your own conclusions, and then choose how best to apply them to your own life.
Executive Summary
Quiet week.
Vaccines still work.
Case counts did not peak yet, but positive test rates likely have peaked.
Let’s run the numbers.
The Numbers
Predictions
Prediction from Last Week: 950k cases (+2%) and 9,400 deaths (+25%).
Results: 1.04mm cases (+10%) and 9,290 deaths (+22%).
Prediction for next week: 1.1mm cases (+5%) and 11,150 deaths (+20%).
The rise in cases here is deeply disappointing. However, if we look at positive test rates, we see a different story:
I’m not convinced the number of actual Covid cases is still rising, but that is certainly possible with case counts rising. Schools are going to reopen soon, which may cause trends to change. If things start to get much worse again before November, I’ll assume that was likely the reason.
For now, given we didn’t peak yet, on average I still expect a small rise in cases, if only from increased testing.
Other people’s predictions, Tabarrok calls the peak on August 30:
Deaths
| Date | WEST | MIDWEST | SOUTH | NORTHEAST | TOTAL |
| Jul 8-Jul 14 | 532 | 398 | 689 | 145 | 1764 |
| Jul 15-Jul 21 | 434 | 341 | 732 | 170 | 1677 |
| Jul 22-Jul 28 | 491 | 385 | 1009 | 157 | 2042 |
| Jul 29-Aug 4 | 693 | 477 | 1415 | 304 | 2889 |
| Aug 5-Aug 11 | 705 | 629 | 2181 | 234 | 3749 |
| Aug 12-Aug 18 | 912 | 851 | 3394 | 388 | 5545 |
| Aug 19-Aug 25 | 1291 | 1045 | 4713 | 508 | 7557 |
| Aug 26-Sep 1 | 1578 | 1256 | 5892 | 564 | 9290 |
Deaths are as expected, and I see no reason they shouldn’t continue to follow cases.
Cases
| Date | WEST | MIDWEST | SOUTH | NORTHEAST | TOTAL |
| Jul 8-Jul 14 | 45,338 | 27,544 | 68,129 | 11,368 | 152,379 |
| Jul 15-Jul 21 | 65,913 | 39,634 | 116,933 | 19,076 | 241,556 |
| Jul 22-Jul 28 | 94,429 | 60,502 | 205,992 | 31,073 | 391,996 |
| Jul 29-Aug 4 | 131,197 | 86,394 | 323,063 | 48,773 | 589,427 |
| Aug 5-Aug 11 | 157,553 | 110,978 | 409,184 | 66,686 | 744,401 |
| Aug 12-Aug 18 | 183,667 | 130,394 | 479,214 | 78,907 | 872,182 |
| Aug 19-Aug 25 | 188,855 | 152,801 | 502,832 | 91,438 | 935,926 |
| Aug 26-Sep 1 | 215,502 | 180,441 | 545,847 | 97,480 | 1,039,270 |
Cases haven’t fully leveled off yet due to a rise in testing, so it’s unclear how to interpret this. My guess is that without school we would clearly be at or near the peak, so the question is whether school will change that. My guess is no at least right away, because when we look at last year we don’t see a rise happening in September.
You can see hospital utilization statistics here. The numbers below are from late last week.
Vaccinations
Our two sources are contradicting each other on whether we’re seeing more or less vaccinations than before, not sure why, but WaPo has proven in the past it can’t do math so I’m inclined to believe Bloomberg. Either way, it does seem like it’s not going to be a big increase in the wake of full approval of the Pfizer vaccine.
Israel has moved to a three-dose standard:
Perhaps the word immune is being asked to do too much work.
Vaccine Effectiveness
It turns out Pfizer’s vaccine can survive storage for (at least) nine months.
Bloomberg newsletter’s way of summarizing the blood clot issue, even if you assume the ffect is fully real.
This preprint from Israel is the latest evidence for the new ‘natural immunity is much stronger than vaccine immunity’ position, replacing the old ‘natural immunity fades at the number of days there has been a pandemic plus one but vaccines are super dope and last indefinitely’ position back when that was the convenient thing to back.
I continue to be highly suspicious of all Israeli evidence that claims the vaccines fade quickly or aren’t that effective, because I’ve seen enough Israeli data that turned out to be the result of bad statistical practices and/or that did not make any sense in the context of what we observe elsewhere or what studies elsewhere report. If Israeli data keeps coming back as if it is from a different universe, even when they claim to have controlled for geographic area and age and so on, I can only conclude that either no they didn’t control for the necessary things or something else is unique about Israel and I won’t speculate here on what that might be.
That said, there’s enough evidence that I’m willing to update. I now believe that natural immunity via previous infection is stronger than immunity from vaccination, plausibly much stronger. That doesn’t mean my estimates of vaccine effectiveness are moving down that much, it’s more that my estimates of immunity from previous infection are going up. At this point, personally, if I was confident I’d previously had Covid-19, I’d be treating myself as close enough to fully immune as to be entirely ignoring the pandemic on a personal level, beyond respecting the requests of those around me.
This also feeds back into the model. If we are missing the vast majority of past infections, and reinfections are extremely rare, then our immunity is increasing rapidly, far more rapidly than the vaccination numbers would indicate.
This post is mainly about the question of whether Biden is ‘listening to the science’ properly enough or not, and whether he is ‘undercutting’ the FDA and CDC by using the executive branch of government to set policy based on his model of physical reality and his view the political situation and needs of the people, And That’s Terrible. The tactic here from Very Serious People is that if the President suggests he is going to do anything in the future that hasn’t already been approved and announced by the agencies, or states any information about the world without letting them do it for him, then he’s undercutting them.
It also reinforced that unforced errors and absurd statements are a lot of why things have gotten so muddled, in particular the CDC taking the position that “vaccinated people do not transmit the virus” along with relaxing their masking suggestions, which then established a baseline from which to scare everyone once again, whether or not that was the plan.
The term ‘spoke broadly’ here still left room for updates back from a rather obviously false presumption back to the previous baseline, which could then sound like a horrible new development. And when you get ‘immense pushback’ and you backtrack in response, that’s not ‘of your own accord.’
Good thread analyzing one of the studies that argues for fading immunity, that concludes we should not update much on the study in question. I agree with the reasoning.
Vaccine Mandates
Duke University lays down the law, and promises to remember.
There is a vaccine mandate at the World Series of Poker.
I’m boycotting too. If you ban the sucker from the table why am I even showing up?
The blaster points both ways: Spokesperson for the National Religious Broadcasters fired for statements supporting vaccination.
Various bullets are available to be bitten into, from various sides, and you can draw your own conclusions.
Are there vaccine mandates I am definitely opposed to? Yes. Yes, there are (news article that notes decision was then reversed).
My understanding of custody law is that this is how it works in everything, all the time. The mother having a damn good reason doesn’t matter, because ‘best interests of the child’ as determined by whim of the judge is all that matters. Essentially the judge decides whatever they want, for any reason they want, there are no rules about what is relevant, and we justify all that with ‘best interests of the child.’ Which often amounts to something isomorphic to ‘I didn’t like their stupid face.’ And the judge could mandate actual anything as a condition, and they often do, and there’s nothing you can do about it. If you don’t comply, or the judge continues not to like your face, well, sorry, you don’t get to even see your child.
The people publicizing the decision as a great idea are another matter, but one can hope that they are from the same portion of the onlineverse for which such expressions are no surprise.
May I suggest that perhaps we can repeal the mandate of non-vaccination more than five minutes before it makes sense to impose a mandate? Anyone?
There’s the argument that vaccine requirements and punishments to the unvaccinated represent an unprecedented and dangerous expansion of governmental powers and violations of freedom. Another argument is (aside from places where there are calls for coercion to stop people from making private choices on who to associate with) that what such violations mainly do is highlight existing patterns of violations and the systems behind them, and make them easier to notice, by creating clashing intuitions and jolting people out of acceptance. It’s a new intuition pump.
Mask and Testing and Other NPI Effectiveness and Mandates
A thread discussing new evidence on effectiveness of masks via interventions in villages in Bangladesh, a post linking to the source, and the full paper. Funding came from GiveWell, because the world is small. Data needs more analysis to translate it into good effectiveness numbers, as these situations get complicated quickly. If you see a given reduction in cases over eight to ten weeks, how do you take into account compounding effects over time, and factor in control system adjustments, and measure how much of infection is within-village versus across villages? Also worth noting that the intervention’s effect on Covid case levels (along with its impact on mask wearing) faded over time, some of which I’d speculate was due to running out of usable high quality masks.
Here’s another thread on the topic. Gotta love this note:
Naturally, there’s plenty of ‘masks work!’ energy to be seen in response, and yes this makes it clear that masks definitely do help somewhat, especially with proper (in this case surgical rather than cloth) masks, with the impact concentrated among the elderly.
Is that because the mask wearing got concentrated around the elderly, which would make total sense from the perspective of the villagers trying to help save lives? Which would imply very different conclusions about what caused what and how.
I also worry about multiple hypothesis issues here, on top of the other concerns.
It’s also worth noting that this week we have a new study that KN95/N95 masks offer superior filtration to surgical masks, which matches my priors, so the upper bound on effectiveness here is higher than what you’d find with surgical masks, especially given that cloth masks were much less effective.
This was a good study and I’m happy we have it, but I’m at a loss trying to translate these results into how much masks work in terms of a given exposure with any confidence whatsoever. I don’t think we can do this:
Ben updated from the study that masks were more effective than he thought, whereas I updated that they were likely somewhat less effective than I thought, which is a good sign since previously my estimate was (and still is) higher than Ben’s.
There are scenarios where mask wearing puts us ‘over the line’ and Covid gets locally suppressed, resulting in 95%+ reductions in cases. There are other scenarios where masks don’t do this because people adjust behavior or they aren’t enough, and the number of cases is mostly unchanged. And we can’t go from X% reduction here to a Y% reduction in chance of an individual transmission without doing more work.
A hard to move object met a hard to stop force. It looked like this.
Score another one for incentives. Football player Isaiah McKenzie is fined for not wearing a mask. Responds by getting vaccinated to avoid this. Posts his vaccine card to make sure everyone knows it.
CNN is claiming ‘we know’ that masks are 95% effective when used properly. Which is odd, because I most certainly do not know that.
Denmark decides they are sufficiently vaccinated, lift all Covid restrictions. This is the way.
Remember, incentives matter:
Vaccination rates and international travel restrictions are not correlated, which is unsurprising since travel restrictions in the current situation are the goggles and do nothing.
As a good example of the rules being Obvious Nonsense:
Or we can keep it in the country:
University limits payments by professors for mask wearing by students to $50 maximum, preventing many win-win transactions. Others frame this differently.
One 88-year-old professor quits mid-class over a student not masking at a different university.
No, Virginia, you can’t have your booster early. It’s not mandatory yet.
In addition to mandating vaccinations, Duke also tests a lot, with interesting results (article):
In summary: Duke Sucks.
Yet Duke is not alone. Amherst is barring its fully vaccinated students from trips into town other than to ‘conduct business’ and instituting endless testing and indoor double-mask mandates (news post).
The stated hope is that these restrictions only last a few weeks, but I am skeptical.
Think of the Children
CDC issues guidelines for schools that includes (among other impossible goals) getting actual everyone vaccinated except the people the CDC won’t let be vaccinated, notes that schools are not achieving impossible goals, presents information like this:
This is the classroom that drew everyone’s attention so it’s incorrect to treat it as a typical outcome, but it’s still helpful data.
In case you’re wondering how sane and non-dystopian school policies are these days, I have some news.
“You must keep it closed for the active shooters.” Sure, if there’s one currently at large in the building. I’d do the math here to figure out how many orders of magnitude this is insane but it would be insulting to even bother.
Viva la al fresco! The concrete’s not so bad. I ate lunch like that most days in junior high school, I’d grab pizza or something not as healthy as pizza (which I’ll leave to your imagination) and sit on the steps somewhere. Sure beat what was in the cafeteria. So yeah, this seems completely nuts, but unlike most such nuts things it happens to plausibly leave the children better off. Liquids are also a reasonable choice. Save room for dinner.
Long Covid
A post-length analysis of the threat of Long Covid from someone I trust to be a good thinker, concludes that the threat of Long Covid while not zero is not so large as to distinguish it from numerous similar background risks we take all the time with such matters.
This study in children came out, and yeah, This Reinforces All Of My Priors and all that.
What this did find was a huge pandemic of Long Covid Prevention, which caused a lot of persistently unhappy children:
Imagine if Covid caused this directly and what we’d have done to prevent it, then consider what that implies about what we should be doing.
The main event here is that Scott Alexander has a ‘much more than you wanted to know’ post on Long Covid.
The first thing to note is that Scott views the related news stories as remarkably good, and takes the reports more at face value than I do. Whereas I view the news stories about Long Covid as not very useful, but having slept on it I do notice that they’ve been less sensationalist than one might have expected, so perhaps this is a sign of Scott having good calibration. Stories should be remarkably good as often as they are remarkably bad, unless you think that being good is a relatively unremarkable characteristic.
Let’s go over Scott’s takeaways and reasoning.
This is an important foundational point for Long Covid, which is that Long Covid is not one thing, it is many things, and it is important not to conflate them. There’s generic being-in-the-ICU-is-bad or being-sick-at-all-is-bad, there’s lung damage, there’s inability to taste or smell, there’s fatigue, and all of it is likely a combination of some real effects, some psychosomatic effects, and some coincidental effects that got misattributed to Covid, and also some amount of fishing expedition. When we focus on a particular risk or harm such as Long Covid, we treat it differently than we are treating all other risks.
His next line is that a percent estimate is ‘kind of meaningless’ but he felt obligated to give one anyway, which I think is net good practice but I’m not sure. What I’m confused by is how he uses the data he reports in this section to end up at 20%, since he quotes studies where (Long Covid percent in Covid group minus Long Covid percent in control group) is respectively at most 28%, 12%, 17%, 13% and 13%, two of which lack a control group. If we naively average that we get 17% minus a few percent for the missing control groups, so maybe 15%. Scott seems to be buying that ‘any symptom at all’ is a reasonable standard here, and that asking ‘did you have Long Covid?’ is ripe with false negatives.
For all of these it’s important to note that it’s confirmed seropositives rather than all Covid cases. Most Covid cases likely remain fully undetected. Then again, it’s possible that some of the effects in the control groups could be due to undetected Covid cases.
It’s also important to note that Covid cases don’t happen at random, and even when there are controls the controls aren’t checking for health profiles in detail from what I saw on spot checks.
The 28% comes from asking if patients have ‘at least one persistent symptom.’ N=234, and the outpatients had a slightly higher rate of Long Covid than the hospitalized patient group. Symptoms that counted included diarrhea, runny nose and ear pain. I don’t know if they were typically mild and they aren’t that big a share of the cases, but that definitely says to me ‘fishing expedition.’
He shows the above graph, and some other stats. He then shows this from the third study, Haverfall:
There seems to be a clear line here where the first four symptoms are showing up at a meaningfully different rate in the two groups, but the later five are not with sleeping disorders in the middle and I’m guessing a secondary effect of various other problems. The declines in the control group over time represent them being asked how long symptoms persisted. So it can be taken as a kind of ‘how long does this last when it happens for other reasons’ measurement, and it’s reassuring to know that if you (in general as an example) report headaches for two months, which sounds terrible, that by eight months you’re a favorite to have had the problem go away.
I’d go a bit further than Scott and basically say that I’d treat the breathing problems, issues with taste and smell, and the fatigue as Long Covid, and the other symptoms as presumed to be coincidental or as indirect consequences.
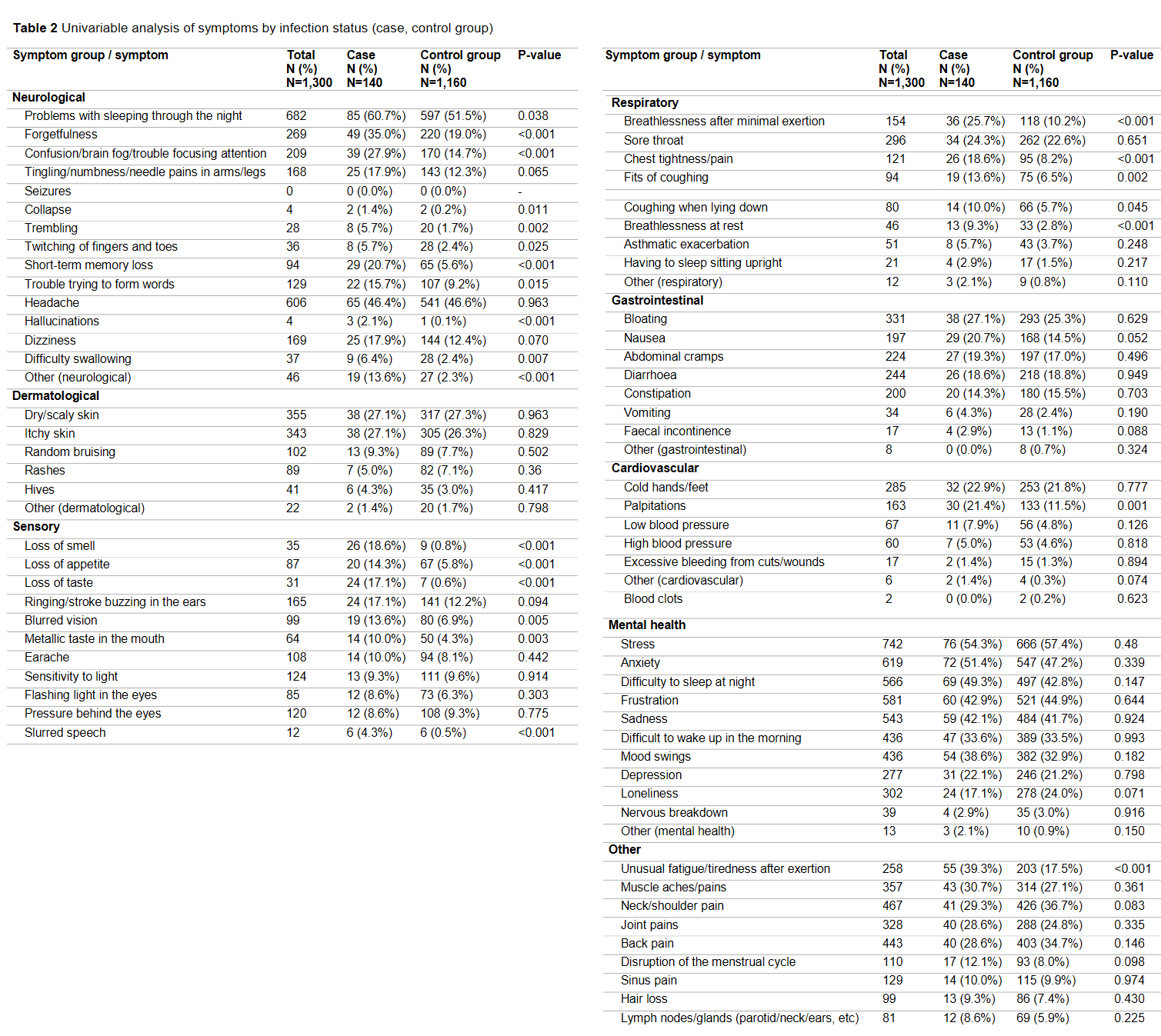
Scott also lists this big chart of symptoms, click on it to read in full, I’m going to highlight the mental health area:
{kind=link}
The control group numbers here are terrifying. This is a crisis. I mean, WTF? Again, it raises the question of what are the effects of Long Covid Prevention on mental health and general well-being, and suggests that they might be far more serious than Long Covid.
When we compare the control group to the symptom group, we find essentially no difference. Symptom group is less lonely, which I’m guessing is directly causal – we should treat more than 7% loneliness as a Long Covid Prevention symptom, along with a lot of the other stuff too.
The symptom had similar amounts of stress, depression and anxiety to the control group, and I’m going to go ahead and question how bad Long Covid can be in expectation if it doesn’t increase any of these factors, compared to the effects of Long Covid Prevention which definitely did spike them a lot.
That doesn’t mean it isn’t real here, in particular the respiratory section looks grim.
Not the most helpful conclusion, but about all we can say given the quality of the data. It seems some people recover, some don’t, and the standards change so much everywhere that saying much more than that is very hard. Scott also points out that the rate of recovery from fatigue due to Covid contradicts the general data that fatigue basically never gets better. No idea what to make of that.
Noted more for completeness than anything else, and that seems right.
As Scott notes, this is important, because the specter of child Long Covid is being used to justify all sorts of stuff.
That conclusion means it does reduce the per-case-at-all rate substantially, since more of the cases will be asymptomatic if one is vaccinated, on top of being less likely to get Covid at all.
This study came out yesterday, and says the risk of Long Covid is cut in half in the vaccinated population versus unvaccinated. My guess is that’s an overestimate, maybe a large one, but that there is some reduction.
This is the headline number that matters, noting that this is conditional on symptomatic Covid rather than Covid, and terrible is being conflated with serious. He notes the disagreement with the first post I linked to, and tries to then do a Fermi calculation of the chance of getting Long Covid if one lived a normal life, and gets very wide bounds, somewhere between 1 in 150 and 1 in 25,000. I think we can safely throw out the upper part of his range, as I think a 10% chance of breakthrough symptomatic Covid within a year isn’t reasonable if you do a little math, and it’s starting at 25% which seems higher than the studies referenced above would suggest, so I think the range here would be more like 1 in 1,000 to 1 in 25,000.
I agree with Scott’s view here that our worries about Long Covid strongly imply the need for more worry about Long Disease in general, and also Long Everything. The previous Aceso Under Glass post emphasized this point, that there’s lots of such risks in the background all the time, and this isn’t an especially big one.
More to the point, Long Covid Prevention has clearly reached crisis levels and really is a big deal, and seems more severe than Long Covid, and a huge percent of the population has this problem, so we need to do what it takes to stop this deadly syndrome in its tracks.
I haven’t yet done a full reading of the Matt Bell post that Scott references. It is long and I do not currently have the time. I hope to read it carefully over the coming week.
I didn’t update much in aggregate, at least for practical purposes.
Long Covid seems legitimate, and worth a nonzero amount of effort to minimize, but my model says it is mixing a lot of things together, is largely typical of what happens after being sick, is protected against by vaccines similarly to how they protect against symptomatic disease, and in many studies they go on a fishing expedition for symptoms then attribute everything that happens chronologically after Covid to Covid.
Thus, basically, ‘don’t do stupid stuff’ still applies, but I have no intention of going beyond that rule, or forming a microCovid budget or anything similar to it.
In Other News
Two ‘heavyweights’ are leaving the FDA and everyone thinks this is because they are mad about pressure from the Biden administration to approve things faster, likely including booster shots. Like in places where the unvaccinated quit, this is both a short term staffing problem and a medium term opportunity for great improvement.
Tyler Cowen has a podcast conversation with Zeynep Tufecki, self-recommending. I found it good, but less surprising than I expected, so I was disappointed. I take that as a sign of proper calibration.
Thread by Nate Silver on booster shots, the evidence in favor of them working, and the need to retire the term ‘no evidence.’
Thread providing color on what’s going on with people using Ivermectin intended for horses. Another thread providing colorful descriptions, rather than explanations.
In response to this, there has been a push to fully bury Ivermectin and to further mock outgroup members by calling it a ‘horse dewormer’ or similar, such as here. I do not think such tactics in any way qualify as helping, and urge all involved to stop using them.
One third of common American deer have antibodies to Covid. Deal was already sealed but this makes it even more clear, we’re not getting rid of this thing.
Ministry of Truth: YouTube gives a strike to a channel for video criticizing anti-vax statements, presumably because it shows a short clip of those statements.
Fluvoxamine preliminarily looks good (as in, worth using, see paper) as a treatment for Covid-19. Not good enough to change general behavior much while you’re healthy, and it’s got enough side effects that one wouldn’t want to use it lightly, but I’d be willing to take it if I knew I had symptomatic Covid. Here’s Kelsey talking about what the results mean and what our priors should likely be here.
An Orthodox Bishop talks about people regretting not being vaccinated.
Australia continues along its path.
But lets down on the gas somewhat in other ways. Such generous, non-dystopian folks.
Max Tegmark reminds a senator we are funding gain of function research, points out it could kill a very large number of people, suggests perhaps we should stop.
(Speaking as a moderator). We’ve varied our policy of frontpaging Covid content over time. Initially we frontpaged Covid content at the beginning of the Pandemic (an exception to the general “timelessness” requirement for frontpage posts) since the info was important and in demand. As thing quietened down, we relegated Covid content back to Personal blog.
Since Long Covid is a topic of great concern for many, I am again making an exception and frontpaging top posts that discuss Long Covid like this one and Long Covid Is Not Necessarily Your Biggest Problem.
As always, you can modify your frontpage tag settings to either ensure you see all Covid posts, never see Covids, or something in between.
This is only confusing if we ignore the elephant in the room. Israel contains God’s chosen people. We should control for this factor in our analyses.
Thanks for this, as always. What does “don’t do stupid stuff” look like to you?
I am having issues seeing the images embedded in the post. When I open them in a new tab, they open to a 403 error:
EDIT: Seems to be fixed.
That’s a problem I’ve heard about on the Wordpress versions of these posts but that’s the first I’ve heard of it happening on LW. It’s been especially bad this week from all reports.
What’s happening is this:
I write the post in Google, using Snipping Tool or Copy Image to grab the images and pasting them into a Google Doc.
I copy/paste the Google Doc into Wordpress. I used to edit directly in Wordpress but their new ‘blocks’ editor is unusably bad unless someone explains why it isn’t. Seriously, wow, it’s bad.
I post to Wordpress.
Post gets copied over to LessWrong from Wordpress.
My current understanding is that this causes the images to remain hosted by Google (and GWS’s comment suggests this is also true of the LW version), and as popularity of the posts has gone up over time, I’m running into rate-limit issues with the images more often.
I need a better solution, with these being the basic conditions:
I can edit in a WYSIWYG editor that can take pasted images directly into the post. Ideally this is hosted online so I can switch computers, but offline is acceptable if necessary.
Wherever I’m editing, once I’m done, I can paste the thing into Wordpress or otherwise easily get it there and post.
Cost in setup time and dollars is ‘reasonable’ in context.
There are other features I’d like, especially better comment formatting/threading, but they’re not important.
Any suggestions? This seems like a crowd that would know what to do here. Also, mod team, should this be happening to the LW version too?
When you drag-and-drop images into LW posts (or paste images from the snippet tool), we upload them into our own CDN, so one option here could be to write the post in the LW editor, and then copy them over into the Wordpress editor. My guess is the copy-pasting should work pretty well out of the box.
I checked and all the images are hosted on googleusercontent.com which is a subdomain that Google uses to hold third party content. The images are probably getting rate limited, as the system serving them was designed to prioritize Google content and not user generated. The practice is usually called hotlinking and that’s why the server started to rate limit. I recommend that you try and host the images on your own Wordpress. Otherwise, maybe throwing Cloudflare in front of your site as a caching layer might be an easier solution.
(Disclaimer: I work for Google as an engineer, but I’m very far away from this system.)
So I’d put the images on Wordpress except that would require using their editor to do so, and their editor is a walking dumpster fire. I could try to reclaim the old editor by using a plug-in but they want $300/year for that, which seems pretty extreme (I’d do it if I couldn’t find any other solution I suppose, it’s not THAT much money, it just stings quite a lot). Cloudflare at $5/month seems better and potentially gives better performance. Can anyone confirm whether this would be a good idea?
Is the Wordpress editor so unusably bad that it’s unbearable (like >$300/year of annoyance) to use it just for swapping in the images? (That is: do what you do now, except that after pasting it in from the Google doc, you go through and do whatever you need to do to change each image from a hotlink to googleusercontent.com into a thing hosted by Wordpress—which in an ideal world might just mean copying each image and pasting it on top of itself, though no doubt Wordpress have found a way to make it much more painful than that.)
If it’s literally that, then it’s on the borderline. If it’s harder, then yeah, it’s that bad.
What does the $300 plugin do that “classic block” doesn’t do? I just edit my posts inside a single classic block, which seems to be identical to the old WordPress editor, including the ability to directly edit the html.
I’m sorry Zvi, but I’ve now realized that you are running on a wordpress.com subdomain. You won’t be able to use Cloudflare, unless you upgrade to the Wordpress business plan (£20 a month) so that you can install plugins.
I don’t have any simple and effective ideas for what you could do, other than putting a call to action for somebody who has more Wordpress experience to help you migrate to a more sustainable setup.
Many schools that weren’t open/in-person last year will be this year, though.
Thanks again.
Missing link?: “This post is mainly about the question of whether Biden...” (which post?)
https://www.statnews.com/2021/09/01/biden-pledged-follow-the-science-but-hes-fallen-short/