Paxlovid no longer illegal. Excellent. Alas, production will take a while to scale, and right now there are other more pressing concerns.
I thought this week’s headline would be divided over two weeks, but life comes at you fast when cases double every two days instead of every three. I’ve already explained why the CDC Nowcast clearly got ahead of itself and outputted obvious nonsense, which is important for putting together a model, but Omicron is still crossing 50% about now and is well past that in major urban areas.
From this point, predictions get a lot harder, our information sources potentially get a lot less accurate as we run out of testing capacity and (in at least some places) hospital capacity, and reactions become bigger unknowns as well.
I hope to have the Omicron post up by end of day, which will go into my current views on severity (very confusing but looking more promising so far) and spread (which looks less unstoppable thanks to confirming a much lower generation time, I think?) but I haven’t yet had time to sort all of that out and different sources continue to tell different stories.
The immediate, on-the-ground situation is a large jump in cases in many locations, ahead of schedule. This next week is when things potentially get quite bad, and also the first time there’s some chance the graphs mysteriously stop going up for no clear reason, as they did in South Africa and maybe did somewhat in the UK.
I also split off my coverage of the quite bad testing situation into its own post.
Omicron Post #9 will happen later today or failing that tomorrow, but there’s a bunch of developing information and I’m still trying to put it together, so I finished this off first and I’m going to take a break.
Executive Summary
Omicron taking over, cases rising dramatically.
Testing is overloaded, at-homes are hard to find, PCRs are hard to get and slow.
Paxlovid approved but in very short supply for now, Remdesivir study says it too is highly effective.
Let’s run the numbers.
The Numbers
Predictions
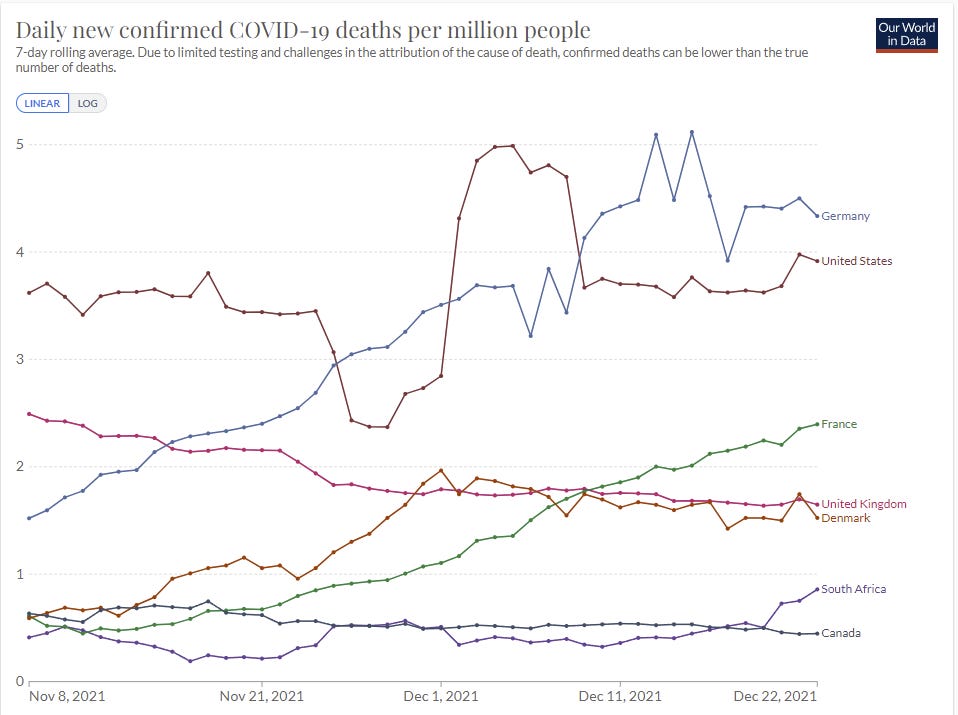
Prediction from last week: 862k cases (+15%) and 9,050 deaths (+3%).
Results: 1.03mm cases (+37%) and 9,203 deaths (+4%).
Prediction for next week: 1.85mm cases (+80%) and 10,200 deaths (+10%).
This would be a new record for weekly cases.
Note that my prediction includes substantial discounting for the Christmas break, and for testing overload and testing reluctance (or reluctance to report the results).
We can compare this prediction market, which has us 50⁄50 to report a record 7-day average by the end of the year. The record used there is 251k cases per day, or 1.75 million, so I’m close to the market value, although I think it’s slightly cheap. Note that they also have the benefit of an extra day.
Last week’s prediction was based on a doubling time of three days. Well, whoops.
Now it gets much harder, because we’re in the adjustment phase and up against the holiday of holidays.
A doubling in one week would be a faster increase than we saw in the UK or in Denmark, but the growth we have seen so far implies far more. Some states did double this past week, while others stayed the same or even declined, because spread is uneven and the United States is large. We’re about to run up against Christmas, with a bunch of people not wanting to get tested right before the holidays and face a quarantine. Others can’t get tested because there aren’t enough tests. Then we’ll face a huge backlog in test processing and reporting. And we don’t know the extent to which behaviors are adjusting, including what happens with Christmas break.
Last year we saw a −20% number for Christmas week, which then bounced back. If there was an avalanche of tests coming in, we might not know until the new year.
So this is the biggest uncertainty week so far, by a lot. It also means that I won’t ‘trust’ the number we get to represent the true state of the pandemic, potentially making the week after even harder to predict than this one.
Deaths
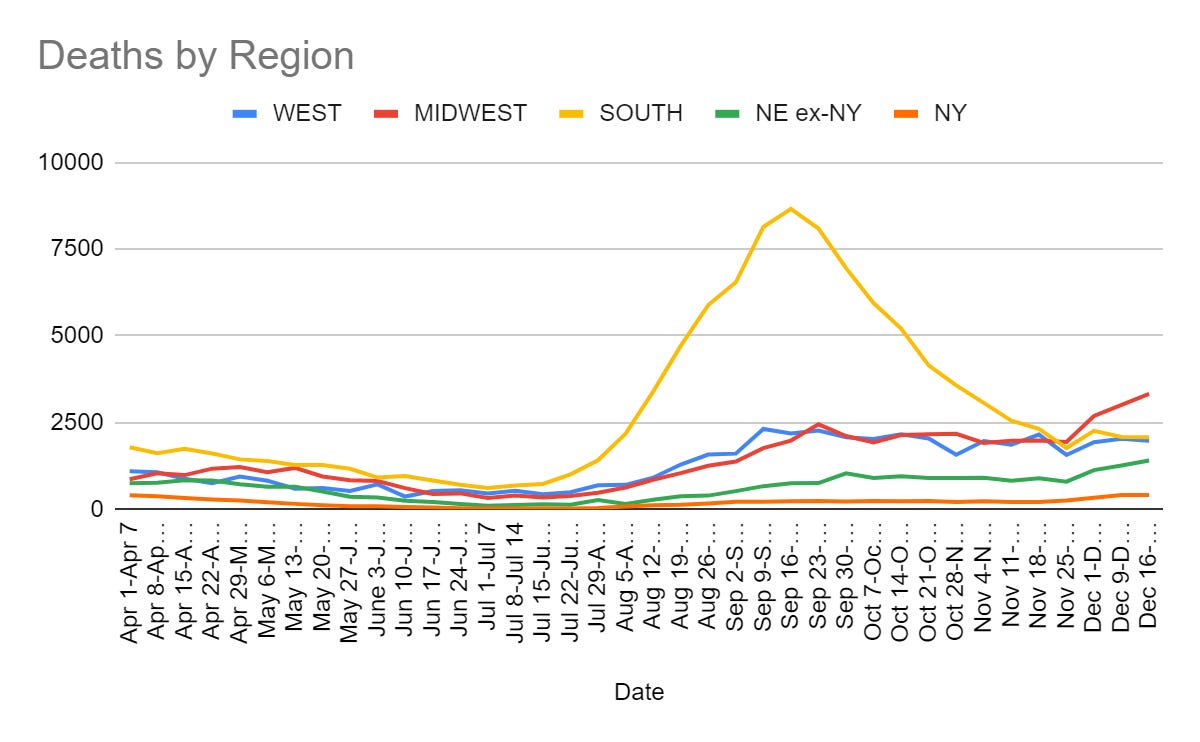
Deaths holding mostly steady most places including the UK:
Cases
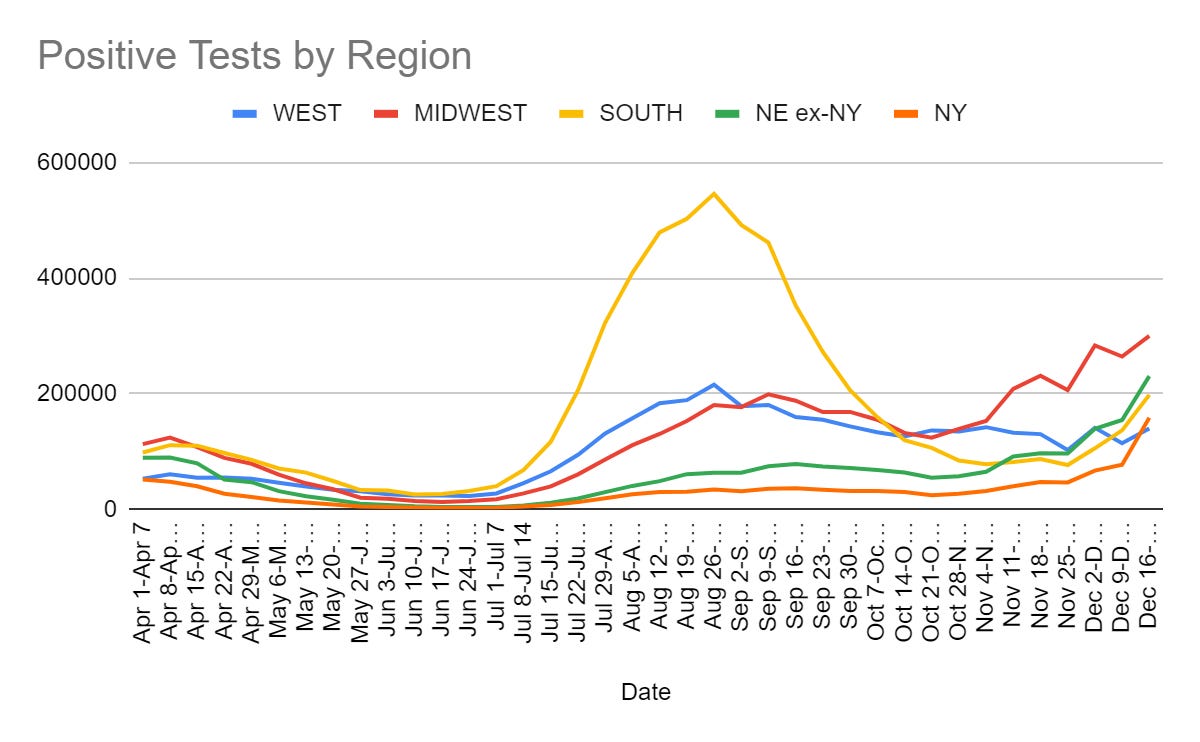

Periodically someone would ask why the Orange line for New York was still on the graph. Now we have more cases than the whole West, about 0.8% of our entire population in one week. That’s only the cases with reported positive tests, and this is probably only the beginning.
The other regions are behind, but they will catch up quickly.
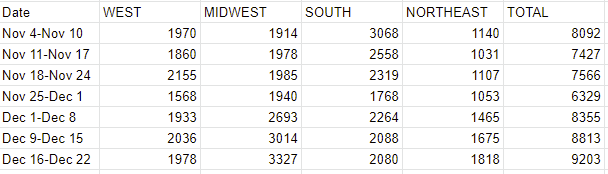
For my international readers, a comparison chart.
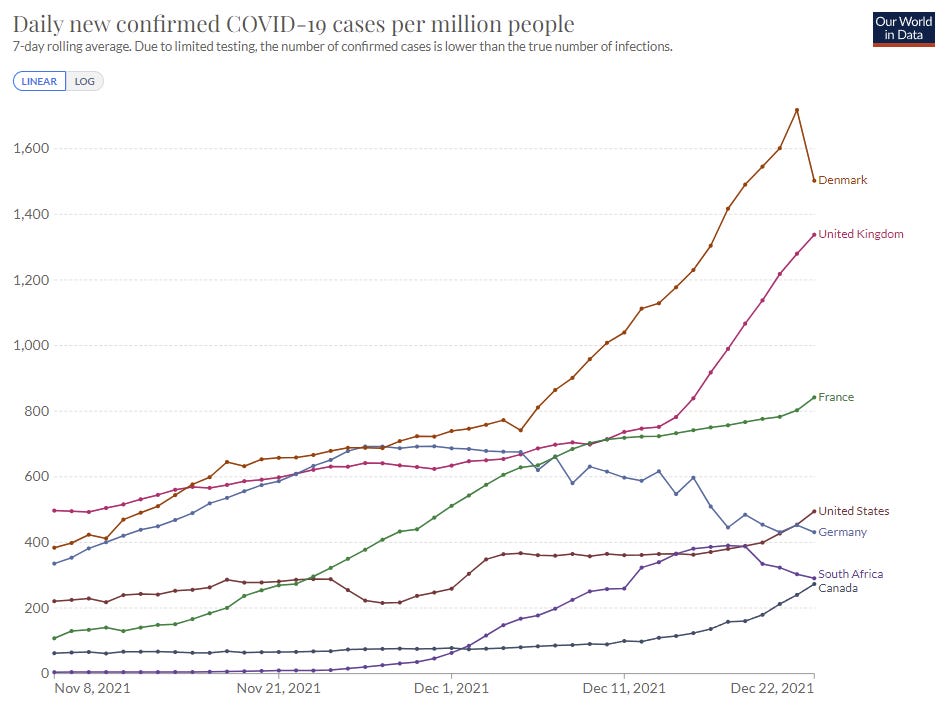
That big final decline in Denmark isn’t real, as the website is recording a big zero for the final day, so ignore that.
Testing regimes are very different. For example, Germany’s death rate has been higher than the UK’s recently, even before Omicron, yet their case counts have been similar and are now lower. South Africa, assuming it peaked, almost certainly peaked with much higher actual case counts than indicated here.
Vaccinations
CDC recommends people not get J&J vaccine if mRNA vaccines are available. There was a bunch of worry that this would become fuel for vaccine skeptics ‘at the worst possible time’ (where the worst possible time is always right now), but that seems to not have happened.
My explanation for why that didn’t happen this time is simple. If mRNA vaccines are available, you shouldn’t get J&J, it doesn’t work as well especially against Omicron, so use the one that works better. Yes, the whole ‘condition that may lead to death’ thing is cited as a reason and is ludicrously overblown, but the ‘is less effective’ part is the part that counts and everyone knows that. What fuels vaccine hesitancy is when decisions are made that treat trivial worries like a big deal in order to not fuel vaccine hesitancy. When decisions are made that make sense, it’s fine.
Meanwhile, someone finally figured out that if the FDA committee is putting its own issues ahead of public health, you can just… not consult the committee. WaPo article here.
These sources are saying ‘oh no, this will hurt our credibility, you’re not following the procedure’ and I would say it’s not a moment too soon and we should learn from this example. The advisory committee is optional. It serves a valuable purpose when you need to understand the information in front of you, but that doesn’t mean you need to invite it to throw a fit for stupid reasons that provides you with no new insight and no new information. The first step to FDA Delenda Est.
Also, here’s a thread pointing out how not-close the math is on whether to vaccinate your kids, it even decreases myocarditis on net because it (get this!) prevents Covid-19 and Covid-19 is kind of bad for you with lots of side effects.
I only have one question about this cat. How do we know it was nine?
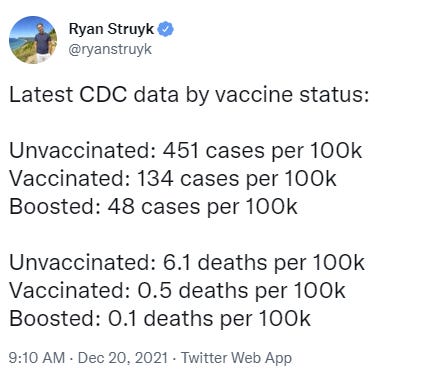
Vaccine Effectiveness
Yep, vaccines still work, an ongoing series, and remember the vaccinated population is older and was much more vulnerable before vaccination.
In other vaccine Not Necessarily the News, from the So It Has Come To This Department, they’re everywhere, so here’s a helpful PSA:
Hail hydra, bitch.
Vaccine Mandates
Yet another indication from Dr. Fauci that booster mandates are coming.
Biden has decided to turn up the rhetoric once more.

In addition to the winter of pain, it’s now an obligation to your country, and also your family and yourself. Them’s fightin words.
Fluvoxamine Remains Slightly Socially Awkward
There is also at least some risk that they’ll refuse to fill your prescription, but mostly the problem is that doctors aren’t prescribing it.
Why? Lack of knowledge, sure. But mainly mild social awkwardness, of course.
Scott Alexander explains the situation in an exceptional piece.
It has it all. You’ve got the scientific case for the drug, which seems very solid. You’ve got the FDA being so dysfunctional that they have no idea how to proceed with approving Fluvoxamine for Covid-19 because there’s no pharmaceutical company looking to profit off of it that can guide it through (although it looks like there might finally be a solution to this after many months, maybe). It’s got mild social awkwardness leading to lots of hospitalizations and deaths, called out for its central role, along with Scott going over how even he struggles with this and sometimes comes up short. You’ve even got a call to do the obviously correct thing.
On to the main event. Paxlovid!
Paxlovid No Longer Illegal
Today, the U.S. Food and Drug Administration issued an emergency use authorization (EUA) for Pfizer’s Paxlovid (nirmatrelvir tablets and ritonavir tablets, co-packaged for oral use) for the treatment of mild-to-moderate coronavirus disease (COVID-19) in adults and pediatric patients (12 years of age and older weighing at least 40 kilograms or about 88 pounds) with positive results of direct SARS-CoV-2 testing, and who are at high risk for progression to severe COVID-19, including hospitalization or death. Paxlovid is available by prescription only and should be initiated as soon as possible after diagnosis of COVID-19 and within five days of symptom onset.
Here’s the Stat News article on the approval. Here’s Some Weekend Reading’s coverage. Pills are on the way, if at first in limited quantities. It has begun. I also got a report on Twitter from the UK of someone who was potentially able to get it for their mum even before USA approval, so it’s already doing some good. It also seemed like the logistical arrangements were solid, which is an important potential point of failure.
Eric Topol calls upon us to use the Defense Production Act to speed up production of Paxlovid, now that it’s been approved (or at the time, clearly about to be approved) rather than addressing the problem that it only just got approved now, or suggesting the obvious first thing of putting in bigger orders and paying more money. The reason this isn’t ‘available to all’ are the barriers put in place and the lack of reliable willingness to pay.

Capitalism Solves This, all we have to do is pay. Pfizer even said they’d license to others, so this should (have been and should still) be a relatively easy one.
I myself made a few inquiries to people who might potentially be able to move the needle, but I came up empty. I didn’t push as hard or follow-up as much as I could have, and I’ve taken to asking myself why. My answer is that I didn’t have the felt experience that I could make a difference if I had some gumption and started playing to win the game. And I didn’t have that same sense of no, this is on you, someone has to and no one else will that I get at some other times, even though I knew damn well no one else would.
Instead, I was largely playing to just play, to say that I’d played at all. I was open to seeing a path forward, and tried a little to find one, but didn’t look that hard. Not good enough. Unacceptable. Better than nothing? Sure, absolutely, better than nothing, 99th percentile effort there. Did I have a lot of writing to do and a day job and a family and no first-order connections to anyone relevant? Yep.
But so what? All of that doesn’t count. Do, or do not. Either you shut up and do the impossible, and cut the enemy, or you don’t. Was this actually impossible from my position? I don’t know. But I also didn’t properly (f*** around and) find out. And this is my apology for that.
Now, a month later, it seems much more real to me that I might have been able to do something. So maybe, hopefully, next time, when something looks as tractable as this did, with as much on the line, I’ll use the try harder. And maybe some of you will use it too.
It is always a valid comment to ask me, so what are you going to do about it, punk? Even better is suggesting what it is I might do about it, but we have to start somewhere.
We have the doses we have. What are we going to do with them? We’re going to divide them among the states apportioned by population, and you can track that here. There doesn’t seem to be any adjustment for conditions in each state, and there definitely isn’t the ‘these states voted for me’ adjustment we saw from the previous administration. What will happen once those doses get delivered? Who gets them? We don’t know this. We only know the first stage.
A factor of three in a month is good, but not remotely enough. Proportionally to cases, it’s likely to be less not more.
In addition to the big good news, you know what else is legal? Remdesivir! And there’s a new study saying it’s 87% effective in reducing hospitalizations in high-risk patients via outpatient treatment.
Everything’s coming up treatments. Imagine if we acted like we cared.
This is The Way
It is all too rare how often the systems we have actually take care of people, and we can all use some good news, so I’m going to share this tale from NYC in full. This is The Way.

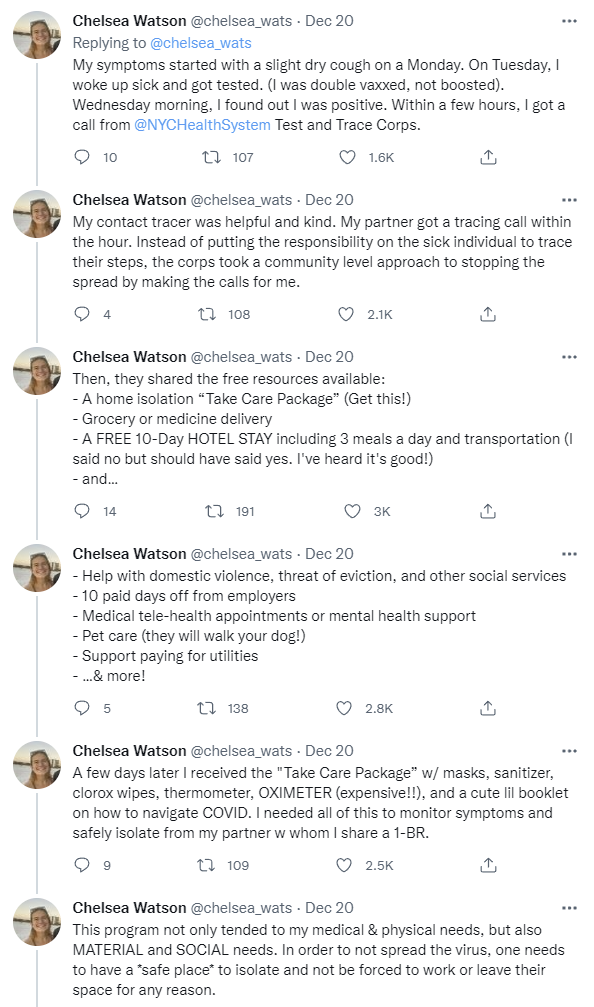
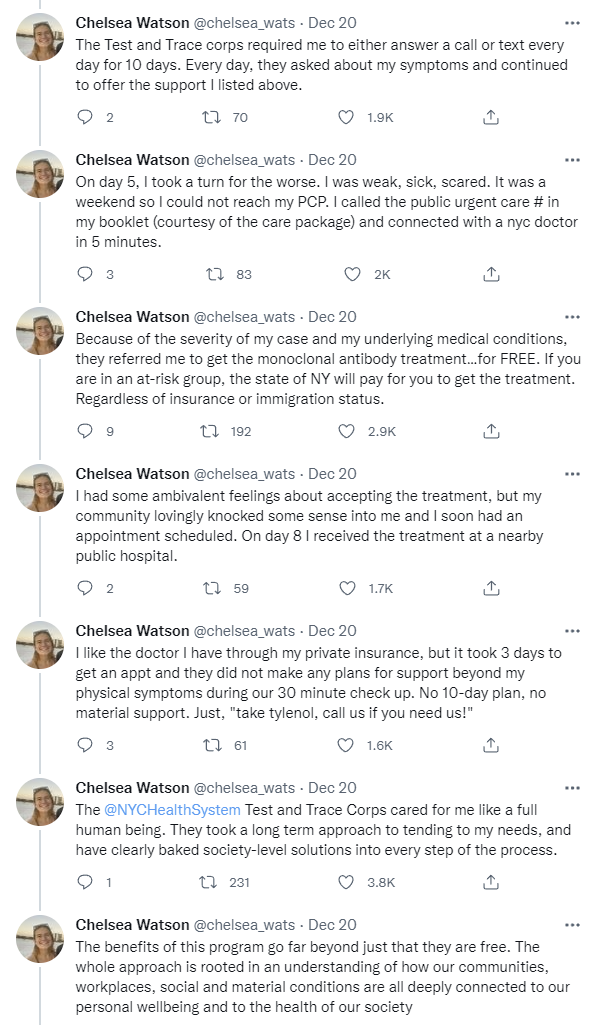
A program like this asks what would actually help solve the problems, for the sick individual’s health and social well-being too, to help them stay isolated and to help others realize they are infected. At least in Chelsea’s case, it focused on what mattered, and it got it done. Everybody wins. Yet we don’t talk about this almost at all, because authorities are terrified of what would happen if we focused on mitigation and helping those who are ill, instead of trying to force people to alter their behavior.
Flying Home for the Holidays
A lot of people have asked about traveling home for the holidays. It’s a little late to talk about it now, but I will reiterate that flying in an airplane is not a risky activity, and that this Bloomberg headline was almost certainly true (risk of everything is at least doubled, why would planes be different) but from a very low base rate, and it wasn’t based on anything beyond the logic above.
So this:

But also still this:
On most planes, the air exchange rate is approximately every three minutes and 75% comes from outside the plane, meaning that only 25% of cabin air is recirculated.
“The 767 and 777 both removed particulate 15 times faster than a home … and five to six times faster than recommended design specifications for modern hospital operating or patient isolation rooms,” the study continued.
What is risky is being at the airport. That’s an indoor interaction with a bunch of strangers potentially lasting hours, and that’s where your risk is when flying. Plan accordingly.
What is it about airplanes that demands ludicrous amounts of both actual safety (e.g. no plane crashes) and also security theater (e.g. the TSA), and now the masks? Is it purely that it’s profoundly unsettling to be flying through the air because that’s something humans aren’t supposed to be doing? Or is there more to it than that?
NPIs Including Mask and Testing Mandates
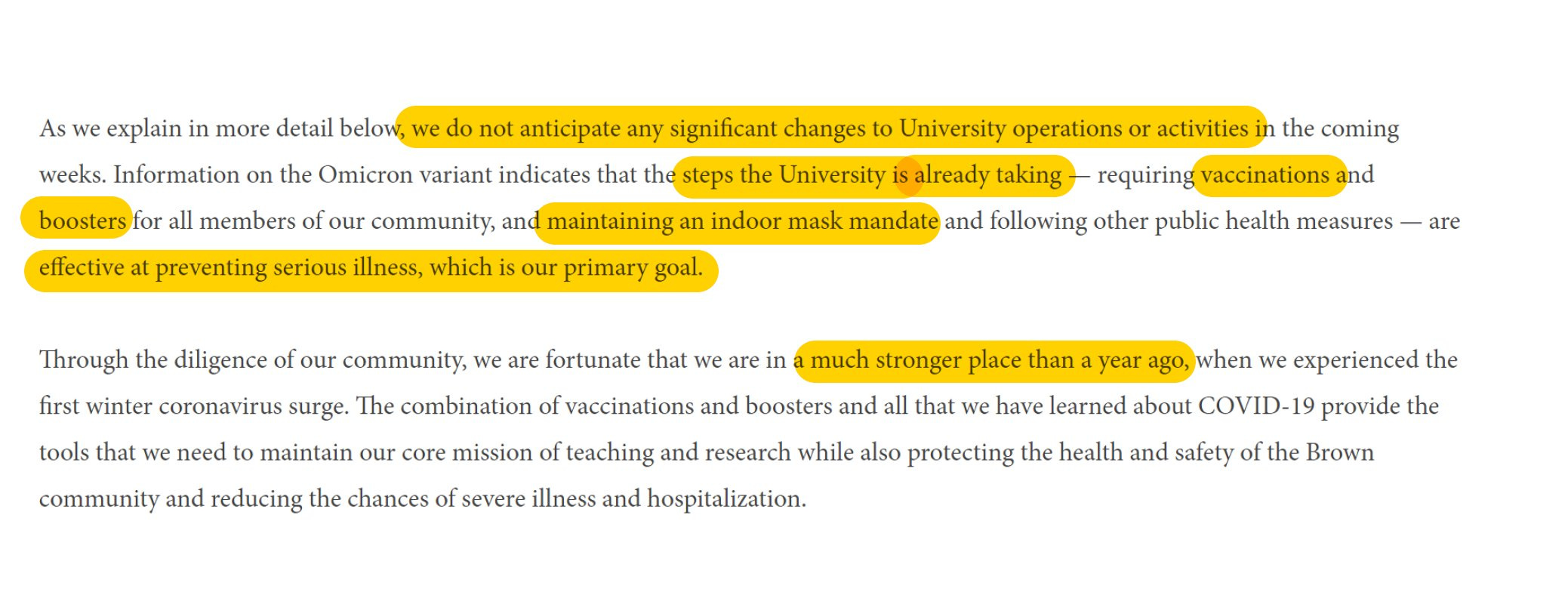
This seems right in terms of who restricts things when.
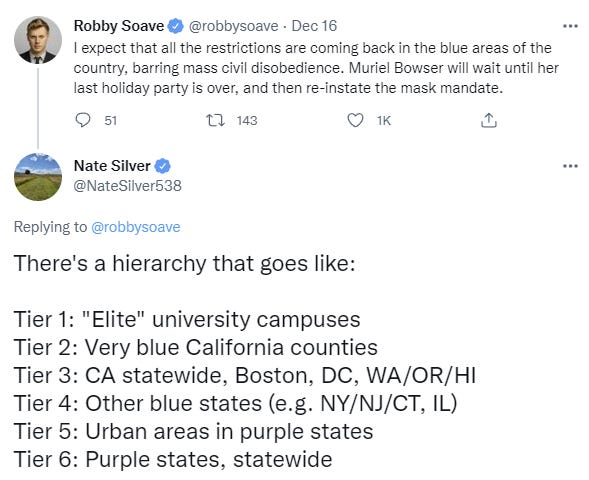
As noted below, Brown University isn’t taking steps, so even Tier 1 isn’t uniform. In general we’re not seeing much movement. Boston went to a vaccine mandate, but that’s about the only substantial move, and that’s a catch-up move. Washington, DC is following suit as announced yesterday, with one dose required on January 15 and two doses by February 15, in time for the Omicron wave to already be over. I don’t think this will ‘crush the hotel and restaurant industries’ or anything but it also won’t accomplish anything given the timeline.
The NYC Department of Corrections has halted all visits, and there’s a request to do the same for the state. I wonder if it’s the definition of chutzpah to say it’s too dangerous to allow visitors and yet keep all the prisoners locked up.
Sports Go Sports
Omicron is sweeping younger and more active populations first, and has a bigger advantage over Delta in more highly vaccinated groups, and more frequent testing of asymptomatic individuals will catch more Omicron cases.
Thus it is no surprise that professional sports are increasingly dealing with Covid outbreaks, and must figure out what to do. So far, the NHL is suspending its season, while the NBA and NFL (remember: no football, no peace!) are soldiering on.
The problem is that current quarantine rules and everyone getting Omicron don’t mix with playing a bunch of ballgames. This has been especially hard on the NBA, and that was five days ago.
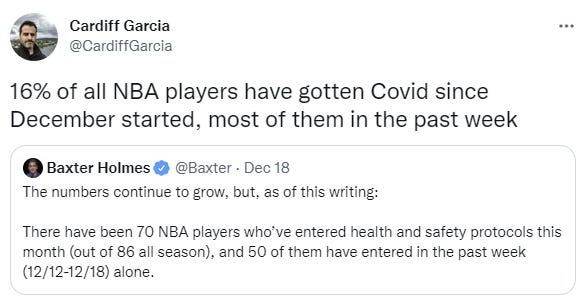
Here’s a post from a week ago detailing how bad things had already gotten, and what their dilemma was. The proposal here is quite aggressive.
The NBA actually has an opportunity here to end the precautionary moment, or at least signal its ebb. If commissioner Adam Silver steps forward and announces that his league is ending test protocols and treating this admittedly terrible disease in much the same way we deal with some other respiratory illnesses, that’s a potential cultural shift. The basic plan would be to test players and team officials only if they’re obviously sick (and sit said players if they test positive). And no more of the contact tracing that’s gummed up work behind the scenes of a highly mobile industry. The message could be simple: Look, we can’t functionally operate like it’s 2020; now that the disease is endemic, and vaccines are widely available, we must move into 2022.
That seems like too much. I wouldn’t have anyone quarantine based on contacts at this point, but if you have Covid-19, you shouldn’t be playing in NBA games until you’re negative. Otherwise the players don’t have time to properly recover, and could end up with long term health issues. If that means signing players off the street for a week, that’s what it means.
As someone who finds the NBA season too long and too monotonous, I kind of want to see teams scramble to deal with outbreaks. If you’re capable of winning the NBA title, you’re not going to be in any danger of missing the playoffs even if your team loses ten in a row while the stars are out, worst that can happen is another few away games, so why not spice things up a little?
Ministry of Truth
Twitter without Jack seems to increasingly have a censorship problem, with Covid-19 being a clear example. Which as always brings out less than the best in response, including people who misquote the policy to make it sound insane, so it’s important to notice exactly what’s happening. Here’s the policy.
The basic principles are thus:
What is in violation of this policy?
In order for content related to COVID-19 to considered violative under this policy, it must:
advance a claim of fact, expressed in definitive terms;
be demonstrably false or misleading, based on widely available, authoritative sources; and
be likely to impact public safety or cause serious harm
In theory that should be fine. In practice ‘authoritative sources’ decide what is ‘demonstrably false or misleading’ based on what they think the public needs to hear rather than what the authorities believe is true, then changing their minds on what is to be considered true when they want the public to hear a different thing instead. Also the authorities are reliably behind in terms of figuring things out.
The requirement to ‘impact public safety or cause serious harm’ is not protective, because what information about Covid-19 doesn’t ‘impact public safety’ or ‘cause serious harm’ given the word ‘net’ is not included there?
Its examples of false claims, they include:
Claims that specific groups or people (or other demographically-identifiable identity) are more or less prone to be infected or to develop adverse symptoms on the basis of their membership in that group;
Older people are a demographically-identifiable group.
And also this:
Tweets that misrepresent or misuse official reporting tools/statistics.
I’m sure everyone who presented the CDC nowcast as fact is about to get suspended Real Soon Now. What does it mean to ‘misuse’ a statistic? Paging Mark Twain.
Finally, yes, here it is, but wait, it’s different and kind of weird:
False or misleading claims that people who have received the vaccine can spread or shed the vaccine (or symptoms, or immunity) to unvaccinated people.
Notice what this doesn’t say, or at least no longer says, which would be that vaccinated people can’t spread the virus. It instead says they can’t spread the vaccine or immunity to others, which they very much can’t, but is the kind of thing some anti-vax people worry about. Nor can they spread symptoms, because that’s not how symptoms work.
What they can spread is Covid-19, albeit less often than those who are unvaccinated. But the policy doesn’t say anything about that when you read it, at least in its current version. It says something else. The something else is so weird that I totally get how one could read it the wrong way, it’s almost a “Paris In The The Springtime” situation, but before hitting publish one needs to check and be sure.
In theory, any disagreement with public health authorities could count under the policy as written, since those same authorities decide what is ‘demonstrably false.’ In practice, I presume they’re not going to use it that way.
In theory the policy can lead to permanent account suspension. For that to happen, you have to mean it. A ban requires five strikes against your account. Mostly accounts will be effectively banned from talk about Covid-19 rather than fully permanently suspended.
Think of the Children
Stanford University was one of the first colleges to announce it was going remote.
Brown University is standing firm and not doing that (full statement).
From The Atlantic and the You Should Know This Already department, The CDC’s Flawed Case for Wearing Masks in School.
Matthew Yglesias reminds us not to close the schools, given what in practice we do when we close the schools (as opposed to noticing school is terrible and fixing it) because it doesn’t accomplish much and does a lot of damage to kids.
The Cost of Prevention
Bryan Caplan asks how one measures an overreaction, calling the one to Covid the most expensive in history.
By my math, the total cost of the reaction for the U.S. was roughly fifteen times the total cost of the pandemic itself. (Similar calculations for Canada here). But that’s fifteen times a genuinely enormous cost of 800,000 lives, implying many trillions of dollars of overreaction.
In contrast: If the total cost of the reaction to shoe bombs was fifteen times the total cost of shoe bombs, the total harm would still be trivial, because shoe bombs themselves are trivial. You could have a 1000:1 ratio, and the sum of the harm of the overreaction would remain moderate. You might argue that a 1000:1 ratio is somehow more intellectually jarring. But if you could push a button to get rid of just one overreaction, you should clearly push the button that undoes more total harm, not the one with the most ludicrous cost/benefit ratio.
I agree with Bryan that what matters is the size of the overreaction, not its size relative to damage done. What I don’t agree with is that you can measure the reaction by comparing it to the damage done. You need to compare the cost of reaction to the damage prevented, in expectation, which is a different calculation.
Otherwise, you end up with ‘why did you spend so much making sure the bridge didn’t fall down, when it clearly didn’t fall down? What a waste of money!’ Or the at-most-slightly less dumb ‘Only two bridges fell down but we spent ten times that making sure other bridges didn’t fall down. What a waste of money.’
In the case of a pandemic and facing exponential growth, the counterfactual pandemic could easily be ‘most of us catch Covid in short order’ and it’s reasonable to compare that cost to the prevention cost. And you need to have model uncertainty of how bad this would get. As it turns out, that still says we paid too much in prevention costs, at least once we were out of the first few months, and definitely after vaccine availability.
Then again, it also means that when you spend over and over again preventing the same one-time harm, or you fight a battle you can’t win in the end, those costs add up, you’ve overpaid that much more. Don’t use your army to fight a losing battle.
Also, you should of course be comparing the costs and benefits of the reaction to a different reaction rather than to no reaction.
But it’s still a key rule of thumb to say that if you spent more preventing X than the cost of X, seems like you messed up.
Bryan also notes that the alternative regimes elsewhere overreacted more than us, which also seems right. That doesn’t let us off the hook, but relative to expectations and the actions of other countries is one hell of a grading curve.
Going forward, there’s value in blunting the gigantic spike that would otherwise be on top of us. But after that, the value goes way down, and it’s time for all of this to end.
In Other News
As a reminder, if you owe someone a great debt, you should pay them back.
A Lannister always pays his debts. America, not so much.

Here’s some examples of good communication about airborne transmission.
A neat little illustration of a transmission pattern.
Hospital capacity is under large strain already in many places, this is one example, and that’s before Omicron.
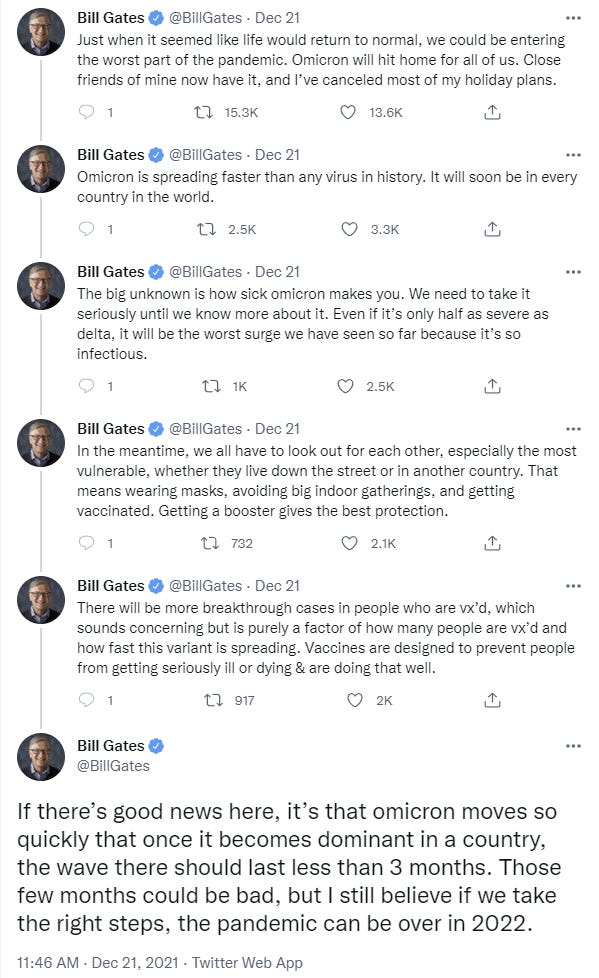
Bill Gates outlines his view of the situation, with four good things and one worry. The ‘worry’ is that people don’t trust untrustworthy governments, rather than those governments being untrustworthy. We’ve ‘learned a lot about how to deal with variants’ except that no we haven’t. We’ve ‘gotten really good at vaccines’ except we’re not moving that quickly to update them nor are we that good at getting people to get vaccinated (although obviously compared to last year, huge win and all that). We’re ‘developing better treatments’ but don’t seem that interested in scaling up and deploying them, and we’ve ‘learned a lot about mandates’ but it’s not clear to me what ‘we’ think we learned, or what that means for next time.
His later Twitter thread isn’t getting anything wrong, but also doesn’t offer useful insight. Seems like given his experience, knowledge and resources, he should be able to do better. I fear the world has taught him that he shouldn’t dare, and that this is as far as he is somehow ‘allowed’ to go.
Not Covid
Robin Hanson once again points out that giving people better health care access doesn’t seem to give people better health outcomes? (Robin’s analysis post here, original paper here.)
Opportunity to purchase insurance led to 59.91% uptake and access to free insurance to 78.71% uptake. … Across a range of health measures, we estimate no significant impacts on health. … We conducted a baseline survey involving multiple members of each household 18 months before the intervention. We measured outcomes two times, at 18 months and at 3.5 years post intervention. … only 3 (0.46% of all estimated coefficients concerning health outcomes) were significant after multiple-testing adjustments. We cannot reject the hypothesis that the distribution of p-values from these estimates is consistent with no differences (P=0.31).
Here is Robin’s very reasonable conclusion, under the circumstances:
So a new randomized experiment on ordinary health residents of India had 6.8x as many subjects as the RAND experiment, and also found no net effect on health. It only looked at the effects of hospital treatment, but to many that is the crown jewel of medicine.
Bottom line: we now have more stronger data that on average, more medicine doesn’t improve health. Though of course for people committed to buying useless medicine insurance can cut financial stress. Update your beliefs accordingly.
Indian hospitals might be much less effective than American or European hospitals, but if there’s no effect that is still quite the thing to explain, and the sample sizes here are large. And we keep finding this same result.
OpenAI is giving their AI access to the internet in a known-to-be-exploitable-way during training. If you thought we were going to get killed by an AGI but at least maybe we would die with dignity, this is the exact opposite of dignity. I know many of my readers, especially new readers, aren’t that up on or invested in the question of AI Safety, but even a completely average person should be able to understand why rule number one is ‘for the love of God at a bare minimum you don’t give your AI access to the internet,’ seriously, what the hell. Could we at least pretend to try to take some precautions? It’s almost as if there are forces pushing towards OpenAI demonstrating that they couldn’t possibly care about safety. And I do appreciate the clarity. It helps one plan.
Article on superforecasting, and current chances of a Russian invasion of Ukraine according to the not-real-money prediction markets that aren’t afraid to go there.
Elon Musk offers a standard list of cognitive biases, so the next time you want to refer to them you can use him as a source, and hopefully all related stocks will go up.
While I agree that giving your AGI-in-training access to the internet is quite possibly a “you lose” style of mistake, I… feel like there has to be some line, and OpenAI explicitly mentioned that they thought they were on the “it’s fine” side of the line, and that treating the situation like they aren’t pretending to try to take some precautions is a mistake.
I think there’s a deeper argument that you might be trying to ‘imply by italics’, or something, which is that there’s winner’s curse reasons to think that dangerous research will be done by the people least able to assess the danger of the research. Also, specialists in a field might not see a reason to do society-wide cost-benefit analyses, instead of local cost-benefit analyses (which will probably diminish the scale of costs more than the scale of gains). See coronavirus research happening in a BSL-2 lab, for example.
But as written this paragraph sounds like “as soon as you start thinking about AI, you should just unplug your computer from the internet, regardless of what program you’re running.” Which… I can sort of see the case for, but requires more explained inferential steps than you’re laying out here to seem reasonable.
(Just want to note that I’m reading every one of these Omicron posts, thanks for them all.)
On the 26th I’m flying Manchester UK to SFO California, with a change at NYC. I understand that the flights are way less risky than the airports, but… well, I’ve got a P3 mask (this one) that I’m planning to wear the whole time except when I’m outside. It cuts into my ears and makes it hard for me to relax. My belief from microcovid.org is that it cuts my risk 20x, similar to (or stronger than) getting a full vaccine.
Anyway, does anyone think I should take it off for the flights, go down to N95, and just wear the P3 in the airport? That’d be a relief but currently I’m expecting sufficiently large numbers of passengers to have Covid (e.g. 5%) that I’m planning to wear it the whole way.
(Also want to say I’ve been reading them all and am very thankful)
Has your N95 mask been professionally fitted?
I was fitted for a mask and they had FFP2 and FFP3 options (which approximately equal N95 and N99, respectively, iirc), and the fitter said that far more important than the grading was the fit. If you had the higher grade FFP3 but air could leak in around the edge, you’d get less protection than the FFP2. Trying out different models of mask in the fitting I was able to detect the bitter tasting test solution in a model that was deemed to not be a good enough fit but not with the model that fitted me.
So by my model, the big advantage of the elastomeric mask you link to is not that it’s rated at P3 so much as the rubber around the edge should go to the contours of pretty much any face and provide a good seal.
I just shaved for it, leaving me looking like 10 years younger, so hopefully the fit is better.
You know the P3 mask I have specifically has movable filters, where if you squeeze them the air flow is cut off, which means I can do a quick check for a perfect fit. It’s the best mask I’ve ever worn for telling if it fits.
I don’t think I’m anywhere near as good with the N95 masks I’ve worn, I expect the fit hasn’t been very good, and will continue not to be. But I will try better in future. Could just tape it down. I would feel more comfortable with it taped to my face than 15 hours of this P3 weighing me down.
N99/FFP3 is an option https://smile.amazon.de/-/en/Aura-Respirator-9330-Folding-Unvalved/dp/B00VAT74NG/ref=sr_1_3?crid=2FHXM7CKD66WS&keywords=aura+3m+9330&qid=1639930225&s=industrial&sprefix=3m+aura+9330%2Cindustrial%2C73&sr=1-3
This thing is as comfortable as the average N95 mask and does a better job and fitting and filtering then the average N95 mask.
A possibly-useful semi test for fit with N95s and the like is sharp inhalation and exhalation, observing whether the mask sucks in and puffs out.
Also, if you wear glasses then I think a well-fitting mask shouldn’t steam them up.
And yes, I was told being reasonably clean-shaven is important for a good fit.
Thanks, v helpful. I now plan to use N95 plus tape for the planes.
Hm, I think I changed my mind, Microcovid gives me 630 microcovids wearing the sealed P3/P100, and 1,600 microcovids with the sealed N95. (It’s guessing at 3.5% prevalence near me, which is really high.)
Also I wore the P3 for a few more hours and it’s mostly fine, except around the ears.
The 1⁄6 for planes seems way too high.
When I count microcovids for airplanes, I assume people are silent. That makes a big difference.
Good point.
RE Robin Hanson’s post on the health insurance study, ‘Most of the p-values weren’t statistically significant, therefore there’s no effect’ is not reasoning that I generally find very convincing.
I’d rather have them combine all the health outcome measures into a single estimate of overall health. Then we can look at the point estimate of the difference in health between getting insurance vs. not, test if it’s statistically significant, look at whether the effect size is too tiny to care much about or meaningful, and look at whether all of the effect sizes in the 95% confidence interval are too tiny to care about or if some of them are meaningful. Maybe even do a cost-benefit estimate, trying to get the units into something more like DALYs per dollar.
(IIRC, the Oregon study that Hanson mentions in his post did something kinda like this, and the point estimate was that people who got insurance had better health, this was not statistically significant, but the point estimate was large enough to care about.)
Looking at the new paper, it does do a few different analyses of effects on health outcomes, but doesn’t say much about them. They call health outcomes a secondary measure and give just these two paragraphs of results in the text of the paper:
So they did calculate a single overall effect on health, which they say elsewhere was “the average of z-scores for individual health outcomes” (that seems like an adequate way to do it but not the best, since it ignores the importance & noisiness of each measure, and the correlations between measures). They say that the effect on that overall health index was not statistically significant, but they don’t say anything about the effect size or confidence interval (maybe there’s something in the appendix but I can’t find find anything about the index in Table A6 or A7).
How do we tell what the Omicron post is? In general?
Confirming—that’s a negative 20%?
Yes, 20% below previous week, which was clearly a reporting issue.
I have always wondered about this. Flying might be a thrill but it is a weird thrill.
“Also, here’s a thread pointing,” etc should probably contain a link.
One of the differences between Germany and the UK is that we have in Germany three times the amount of ICU beds and are thus likely to put people into the ICU that wouldn’t get there in the UK.
It’s possible that people get put on ventilators that should not be on ventilators and die as a result?
I find the ‘ICU access is bad actually’ to this extent unlikely to be the explanation? Even if it’s bad, could it possibly be big enough?
I just wanted to offer it as one hypothesis.
A priori we would expect that the higher ICU beds help with reducing the number of deads, the fact that this doesn’t happen alone is remarkable.
Looking at cumulative numbers per population on OurWorldInData:
As of Nov 21, Germany had performed 1001 tests per thousand people, vs 4697 for the UK.
They’d found 64.6 cases per thousand vs 144.6 in the UK.
The cumulative CFR was 1.84% vs 1.46% in the UK. Checking 3 weeks later for lag effects, Dec 12 was 1.62% vs 1.35%.
My guess is that all else equal, the UK has had a similar or higher IFR, but is catching a larger fraction of infections. In general. I’m not going to try to tease apart the differences in the current or recent situations.