General notes: This is a hard problem. You will not be able to give a useful answer by skimming. I couldn’t include all relevant information because there’s just too much; I’m happy to answer any questions in the comments.
Biomedical context: I’m 25 and otherwise healthy, nonsmoker, active, good cardio endurance, normal weight, no STDs or potential exposure, etc.
[ Edit: As of 26 October 2025, an acquaintance has suggested the original problem might have been related to some injury from a Covid test. I’ve become suspicious that they’re right, and some piece of detritus was left in my right nasopharynx when I was swabbed in 2020, and may still be there. It would explain where the bacteria [which started causing symptoms in 2021] came from, and the occasional scratchy feeling in that area, like the one I keep getting now that I’ve rinsed my sinuses 5x over the past 3 days with NeilMed/[distilled vinegar] solution. Not sure though. ]
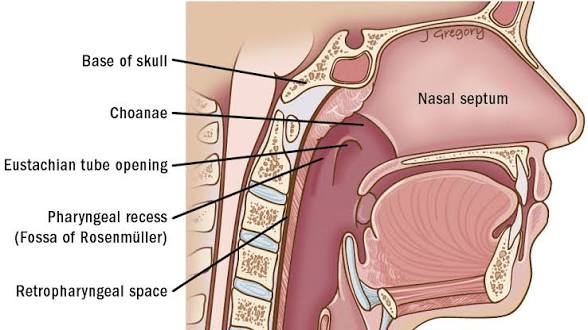
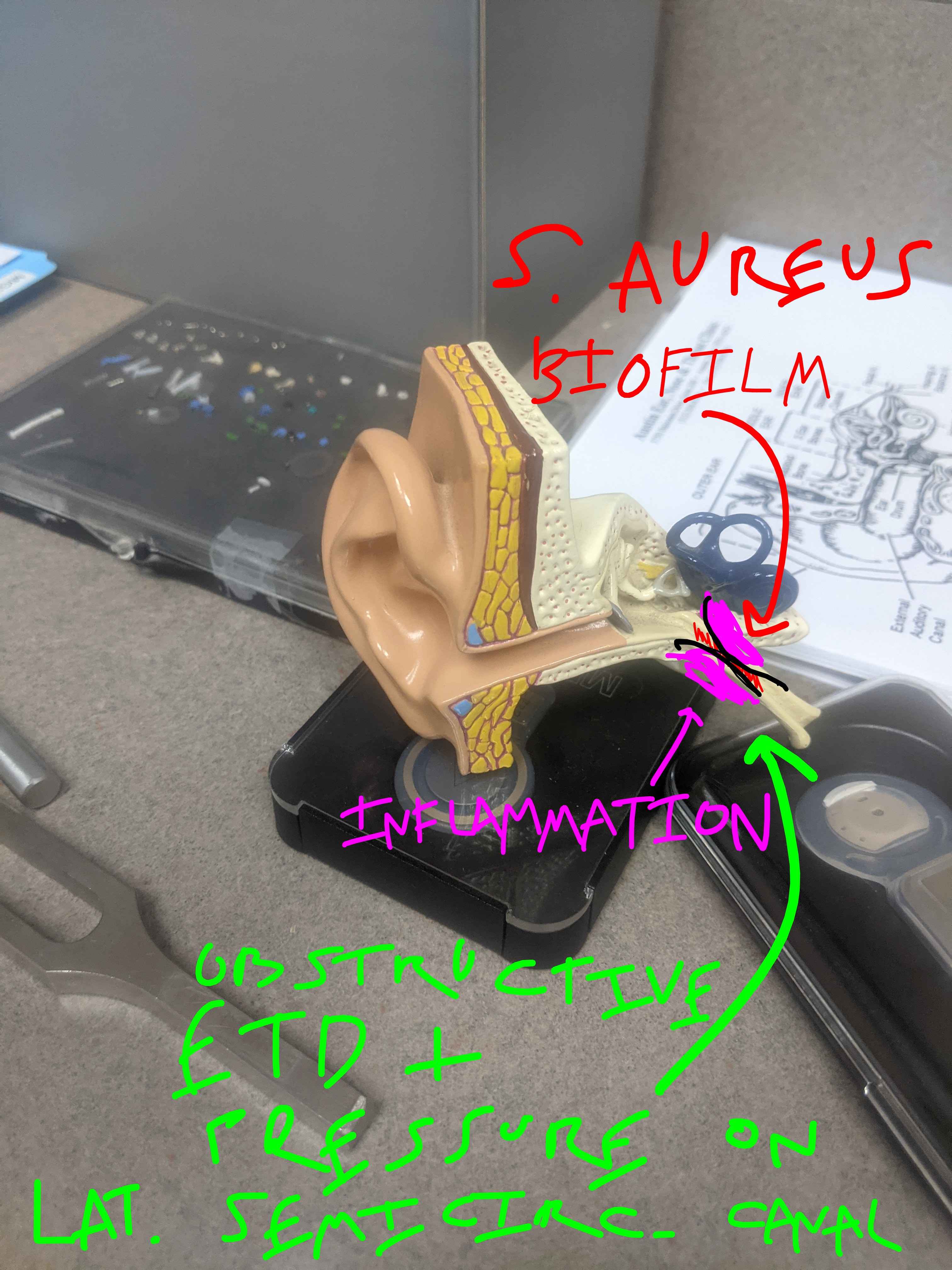
My staph nasopharyngeal biofilm has become aggressively clonal, repeatedly and, for the last two months, perpetually, infecting my skin, ears, and eyes, as well as giving me Eustachian tube dysfunction and vertigo by perceptibly inflaming the nasopharynx itself [ an unusual symptom, but one I’ve been experiencing with more or less monotonic increase since March of 2021 ]. It is also antibiotic-tolerant, which for staph means it has a barely-alive low-ATP quiescient phase that reactivates and recolonizes my tissues after every antibiotic dose wipes out the currently-metabolic-phase cells and temporarily alleviates my symptoms. Tried: neomycin, garlic, ofloxacin, doxycycline, azithromycin, sulfamethoxazole/trimethoprim, augmentin, mupirocin. Now been on the latter three antibiotics and washing skin with chlorhexidine for 6 weeks and counting, to partially suppress skin pustule formation and middle ear blockage. [ This is not good for me. ]
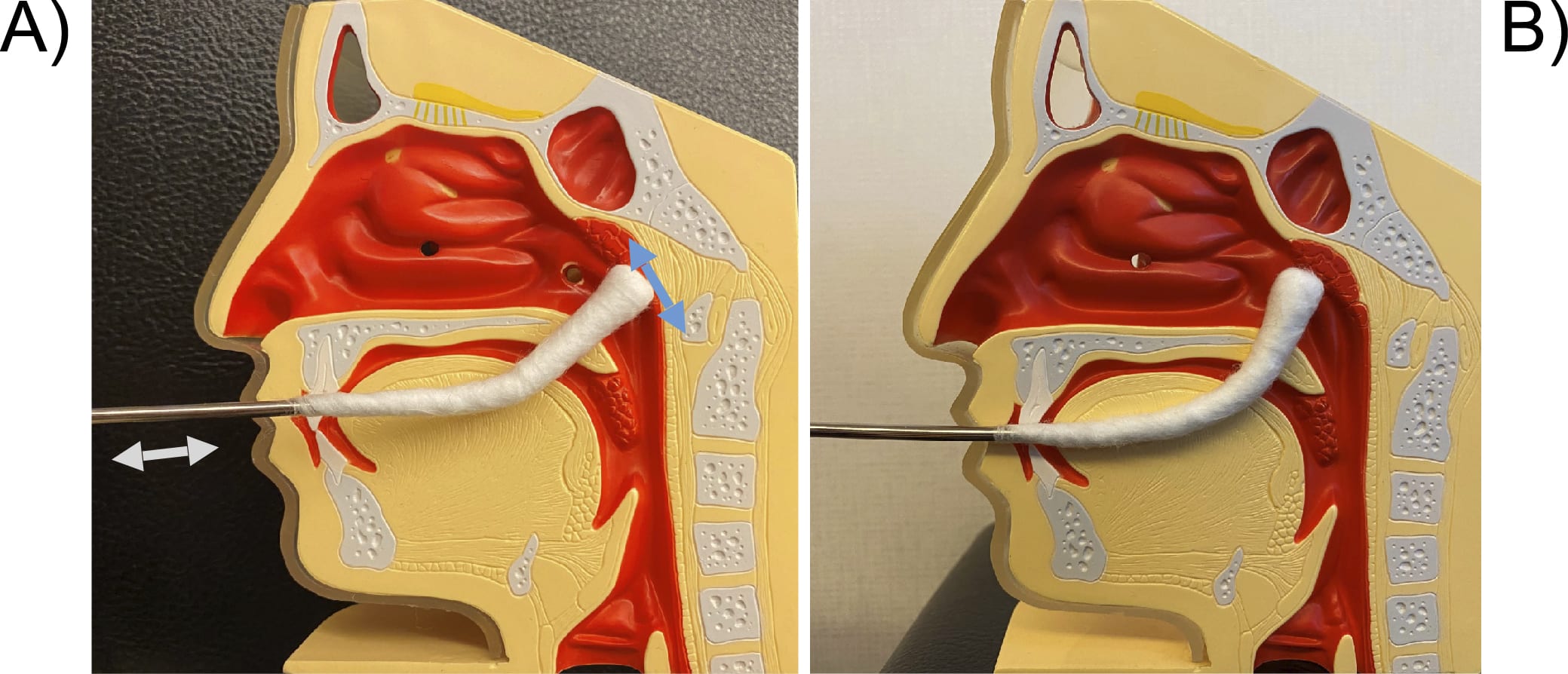
I am already [re]trying gargling sterile saline and diluted vinegar. I will probably finagle nasal washes with those as well, but I instinctively doubt that repeated mechanical clearage with such weak solvents/bactericides will be enough, and I’m concerned I’d eventually wash lots of staph somewhere it shouldn’t go, especially since moisture easily disperses my skin colony. If this was Japan, I’d get nasopharyngeal[/”epipharyngeal”] abrasion [ EAT ];
I’ve already submitted a consultation request with the one clinic in the U.S. that does this. The other obvious option is “biofilm-busting antibiotics”; I haven’t been able to find them on the grey-market sites and I’m on a several-weeks-long waiting list to see an infectious disease specialist who, after the last 20 doctors, will likely dismiss my claims without testing me anyway, if I don’t have grape-sized pustules all over my arms and legs. [ CW unpleasant skin lesions: images of Lorec’s leg pustules. ]
[ My alarmed but overworked GP, who saw the grape phase, maintains my stabilizing antibiotic dose and says anything else is above her pay grade. A previous GP had tried to claim it was fungal; I’d had to source the antibiotics myself. Then the next could prescribe enough doxycycline to clear up my obvious middle ear infection . . . but no more. He said the nasopharynx stuff was beyond his pay grade, and sent me to an ENT who assured me the nasopharynx couldn’t affect balance and all ETD was because of allergies and refused my request to follow up. And on and on . . . x 20. Just saw another one of these ENT chuckleheads a couple weeks ago. Totally different city, totally different state. At first he said the nasopharynx didn’t communicate with the middle ear. I pointed out that it does. He had this model on his table.
“Admittedly the nasopharynx is above my pay grade”, he said. There have been like 6 of these guys at this point. ]
The thing that’s worked the best?
Fresh garlic purée as a nasal spray. Totally cured me for several hours. None of the oral antibiotics have come close. [ But months of Flonase and then months of Nasacort just prior hadn’t done anything, so I know the effect was chemical rather than mechanical. ]
{kind=link}
Am I going to try that again given, you know, agar delivery direct to CNS?
Maybe. I’m getting desperate.
How remove clonal persister staph biofilm from nasopharynx before sepsis? I need to physically get the biofilm out, and then either find some way to kill the persisters [ there are a few experimental chemicals that do this in vitro ], or stamp out the living drainage so rapidly that the persisters fail to repopulate.
Self-EAT? Some antibiotic nasal spray I’ve never heard of? Throat spray? How high should I prioritize trying nasal hypochlorous [ as getting it will be a nontrivial effort for me and most studies don’t find an advantage over saline ]? Self-myringotomy [ risk of CNS infection is way too high, right? ]? Is there something I don’t know about rifampin & co. that means I should expect them not to be as useless as every other oral antibiotic against the nasopharyngeal fortress?
Caveats: this is all vibes based. The following LEGALLY NOT ADVICE is pretty low-risk and easy, but I have no idea if it will actually work. Some people have already tried this (look up Nasal Microbiome Transplant)
Best guess: your nasal microbiome is in a low diversity disease state similar to C. difficile infections in the gut. Hitting it with antibiotics doesn’t work because the staph just resists and rebounds faster than anything else.
What I would do in your situation: use the garlic nasal spray, leave it an hour or so, then (the unpleasant part) put someone else’s snot up your nose to recolonize your nasal cavity with a healthy, diverse microbiome.
The important other question is whether you should come off the antibiotics for a bit. This is higher risk than any other part of the advice (since the antibiotics are for maintenance) but might be necessary: if you stay on the antibiotics, you might just kill off all your brand new microbiome.
! This actually makes a GREAT deal of sense since learning that raw apple cider vinegar contains its own biofilm, which probably accounts for some of how it colloquially helps alleviate insulin resistance [ Horiguti found in 1975 that mechanical nasopharyngeal abrasion restored insulin response in diabetics ].
How did you learn of this class of problem?
C. diff is the classic case, fecal transplants are really well established there as the good treatment for antibiotic-induced infections at this point. I learned about it reading about the microbiome a few years ago.
FWIW I actually also ran the idea past my partner who works in microbial community modelling (though not in anything medical related, they run simulations) and it was roughly:
I should have said, I’d known about fecal transplants being miracle cures per se, that was the main reason I’d been able to come up with that hypothesis for why drinking raw ACV worked better than drinking distilled vinegar.
It just seemed like a non-obvious [ though valid ] inference to make, and I’d been wondering if I’d missed an existing nasal microbiome or general tissue microbiome literature.
But I guess you just had a sensible idea.
Edit: It’s a thing! [ Link ], [ link ]
Talk with rural healers who are doing this now out of necessity.Basically you just want to hit it with as much crap as you can. You may need a lot of crap. There may be fungal involvement, in the nasopharynx as well as the skin [it being known on the skin, though not to what degree], who knows. Pasteurized and distilled vinegar won’t give you brain-eating amoebas used as a nasal rinse, and the acetic acid will still help. But raw ACV likely works better than white vinegar for passive nasopharyngeal abrasion in prediabetics because it’s composed of acetic acid and acetic acid-producing biofilm. Rinse [Neilmed, $12 rinse kit] with [distilled vinegar]-spiked saline, gargle with raw ACV [$1-$5]. The biofilm will try to rebound within hours like it did with the garlic nasal spray, so however you have to, make sure you can keep rinsing.* Wash your tympana with sterile mupirocin-dosed water too, it may drain through the nasopharyngeal mucosa again. There are non-medically-regulated topical biofilm-busters you can get; they may all be too expensive.*Unless the vinegar does nothing, in which case you’ll have to try the garlic again and probably start looking at obtaining some weirder substances.
Then you can do EAT with disposable plastic nasopharyngeal swabs. You will need to do more odd jobs to obtain the swabs. Use the cheapest substances Horiguti claimed in 1975 were equivalent to zinc, and then everyone forgot about for 50 years because zinc was what he’d happened to have on hand.
This person had permanent good results from garlic, so you probably want to get more [because it’s cheap], keep some on hand and if you can make a purée for EAT [less risky than nasal spray and it’s not worth getting time with a food processor for merely the expected benefits of gargling].
The first step is to get used to rinsing with sterile saline. It is safe!!! Don’t let it touch tap water!!! I believe in you!!
All of the above is unless [ reddit user /u/asillybunny ] responds to you, in which case do whatever reddit user /u/asillybunny says.
Just adding to this—have been rinsing with saline for a long time due to nasal polyps. All I do is boil tap water for about 5 minutes and add the required dose of salt+bicarbonate (NeilMed bags). It’s been years now and well, no brain-eating amoebas yet. This in the UK, btw, not sure if other waters can be at higher contamination risk but afaik the amoebas die around 60-70 C.
You might benefit from investigating regimens for eradication of resistant staph colonization, in your case colonization of the nose / nasopharynx and skin. See for example https://www.sciencedirect.com/science/article/pii/S2666524724000405#:~:text=Nasal%20decolonisation%20is%20commonly%20accomplished,skin%20decolonisation%20(figure%203) or https://www.health.wa.gov.au/Articles/A_E/Decolonisation-treatment-for-MRSA . Note that some of these measures require a prescription, and for such I would suggest you consider a consultation with an infectious disease specialist. Note also that measures to remove staph (MRSA) colonization may fail if someone in the household or similar close contact is a carrier and passes it back to you after treatment. Perhaps you could discuss that with the infectious disease doc as well.
I see you skimmed. I have exhausted my options for adult ID specialists in the area except for one, with whom I am on a long waiting list and from whom I don’t have reason to expect much attention. And I’m already using mupirocin for nasal and skin decolonization. The persisters are just too numerous and fast without disruption of the main reservoir. But thanks for the link anyway.
You could try to motivate them to treat MRSA carrier status even if you are not overtly infected by referring to data like this: https://www.jabfm.org/content/methicillin-resistant-staphylococcus-aureus-colonization-and-mortality-risk-among-community . One thing they may want to do first is a swab or two to verify your MRSA carrier status before treatment, so I’d consider stopping the mupirocin and other antibiotics at least a few days before the appointment to best culture things. Best wishes with the pending appointment(s).